








2015-9
Ex-Prisoners’ Perspectives on Prison Drug Treatment in Ireland
John M. Duggan
Technological University Dublin
Follow this and additional works at: https://arrow.tudublin.ie/aaschssldis Part of the Social and Behavioral Sciences Commons Recommended Citation Duggan, John M. (2015) Ex-Prisoners’ Perspectives on Prison Drug Treatment in Ireland. Dublin, Masters Dissertation, Technological University Dublin.
This Dissertation is brought to you for free and open access by the Social Sciences at ARROW@TU Dublin. It has been accepted for inclusion in Dissertations by an authorized administrator of ARROW@TU Dublin. For more information, please contact arrow.admin@tudublin.ie, aisling.coyne@tudublin.ie, gerard.connolly@tudublin.ie, vera.kilshaw@tudublin.ie.
Ex-Prisoners’ Perspectives on Prison Drug Treatment in Ireland
John M. Duggan, BA, B.Corp. Law, LL.B
Submitted to the Department of Social Sciences, Dublin Institute of Technology, in partial fulfilment of the requirements leading to the award of Masters (MA) in Criminology
Dublin Institute of Technology September 2015
DECLARATION OF OWNERSHIP
I declare that the attached work is entirely my own and that all sources have been
acknowledged.
Signed__________________________
Date____________________________
Word Count: 15, 800
ACKNOWLEDGEMENTS
I would like to express appreciation to my supervisor Dr. Kevin Lalor for his steady accompaniment, encouragement and advice. A sincere thank you to the staff of the School of Languages, Law and Social Sciences in Dublin Institute of Technology for their support. To my parents, Ann and John, to whom I owe so much … thank you. To the community of Cherry Orchard, who inspired this study … thank you. To the seven participants in this study who spoke from their heart and asked for nothing in return but that their voice be heard … thank you.
TABLE OF CONTENTS
DECLARATION OF OWNERSHIP …………………………………………………………………………………………………….
ACKNOWLEDGEMENTS ……………………………………………………………………………………………………………….
TABLE OF CONTENTS ……………………………………………………………………………………………………………….
ABSTRACT ………………………………………………………………………………………………………………………………
CHAPTER ONE: INTRODUCTION …………………………………………………………………………………………………..
1.1 Introduction …………………………………………………………………………………………………………………….
1.2 Aim and Objectives ………………………………………………………………………………………………………….
1.3 Summary ………………………………………………………………………………………………………………………..
CHAPTER TWO: LITERATURE REVIEW ………………………………………………………………………………………….
2.1 Introduction …………………………………………………………………………………………………………………….
2.2 Prison Drug Treatment in Europe ………………………………………………………………………………………
2.2.1 European context ……………………………………………………………………………………………………….
2.2.2 Drugs in Prison ………………………………………………………………………………………………………….
2.2.3 Efficacy of prison drug treatment ………………………………………………………………………………..
2.2.4 Profile of Participants in Prison Drug Treatment ……………………………………………………………
2.2.5 Prison Environment ……………………………………………………………………………………………………
2.2.6 Delivery of Prison Drug Treatment ……………………………………………………………………………..
2.2.7 Types of Prison Drug Treatment in Europe …………………………………………………………………..
2.3 Prison Drug Treatment as a Health Strategy ………………………………………………………………………..
2.3.1 Acute Health Needs …………………………………………………………………………………………………..
2.3.2 Fundamental Human Rights ………………………………………………………………………………………..
2.3.3 Equivalence of Care …………………………………………………………………………………………………..
2.3.4 Duty of Care ……………………………………………………………………………………………………………
2.4 Prison Drug Treatment in Ireland …………………………………………………………………………………….
2.4.1 Drug use in Irish prisons …………………………………………………………………………………………..
2.4.2 A Need for Research ………………………………………………………………………………………………..
2.4.3 A Recent History of Prison Drug Treatment in Ireland …………………………………………………
2.4.4 Delivery of Prison Drug Treatment in Ireland ……………………………………………………………..
2.5 Some Challenges for Prison Drug Treatment in Ireland ………………………………………………………
2.5.1 Need for Accountability and Review ………………………………………………………………………….
2.5.2 Unreliable Access ……………………………………………………………………………………………………
2.5.3 Effectiveness of prison drug treatment ……………………………………………………………………….
2.6 Ireland in the context ………………………………………………………………………………………………………
2.7 Conclusion ……………………………………………………………………………………………………………………
CHAPTER THREE: METHODOLOGY …………………………………………………………………………………………….
3.1 Introduction …………………………………………………………………………………………………………………..
3.2 Overview of the Research Rationale, Strategy, Design and Approach …………………………………..
3.3 Research participants ……………………………………………………………………………………………………..
3.4 Data Collection and Procedures involved ………………………………………………………………………….
3.4.1 Interviews ……………………………………………………………………………………………………………….
3.5 Framework for Data Analysis ………………………………………………………………………………………….
3.6 Ethical Issues and confidentiality …………………………………………………………………………………….
3.7 Limitations ……………………………………………………………………………………………………………………
3.8 Conclusion ……………………………………………………………………………………………………………………
CHAPTER FOUR: FINDINGS ………………………………………………………………………………………………………..
4.1 Introduction …………………………………………………………………………………………………………………..
4.2 Profile of Participants ……………………………………………………………………………………………………..
4.3 The Prison Environment …………………………………………………………………………………………………
4.3.1 Prison Culture …………………………………………………………………………………………………………
4.3.2 The Prisoner Code ……………………………………………………………………………………………………
4.3.3 Availability of drugs ………………………………………………………………………………………………..
4.3.4 Prison as an initiation into drug use ……………………………………………………………………………
4.3.5 Benefits of the Prison Environment and Drug Treatment ………………………………………………
4.4 Prison Drug Treatment ……………………………………………………………………………………………………
4.4.1 Person-centred treatment …………………………………………………………………………………………..
4.4.2 Methadone ………………………………………………………………………………………………………………
4.4.3 Stigma ……………………………………………………………………………………………………………………
4.4.4 Staff ……………………………………………………………………………………………………………………….
4.4.5 Drug Treatment Programme ……………………………………………………………………………………..
4.4.6 Fellowship Meetings ………………………………………………………………………………………………..
4.4.7 Access ……………………………………………………………………………………………………………………
4.5 Communication ……………………………………………………………………………………………………………..
4.5.1 Lack of Communication ……………………………………………………………………………………………
4.5.2 Negative consequences …………………………………………………………………………………………….
4.5.3 Importance of Effective Communication …………………………………………………………………….
4.6 Change and the Impact of Policies on Prison Drug Treatment ……………………………………………..
4.6.1 Changes in Prison Drug Treatment …………………………………………………………………………….
4.6.2 Impact of Policy ………………………………………………………………………………………………………
4.6.3 Slow change ……………………………………………………………………………………………………………
4.6.4 Role of leadership ……………………………………………………………………………………………………
4.7 Attitude and Motivation ………………………………………………………………………………………………….
4.7.1 Desire to change ………………………………………………………………………………………………………
4.7.2 Honesty and Integrity ……………………………………………………………………………………………….
4.7.3 Belief in Change ………………………………………………………………………………………………………
4.7.4 Attitude towards prison drug treatment ………………………………………………………………………
4.8 Accountability ……………………………………………………………………………………………………………….
4.9 Conclusion ……………………………………………………………………………………………………………………
CHAPTER FIVE: DISCUSSION ……………………………………………………………………………………………………..
5.1 Introduction …………………………………………………………………………………………………………………..
5.2 Profile of prisoners …………………………………………………………………………………………………………
5.3 Prison Environment ………………………………………………………………………………………………………..
5.4 Healthcare …………………………………………………………………………………………………………………….
5.5 Delivery of prison drug treatment …………………………………………………………………………………….
5.6 Attitude and Motivation ………………………………………………………………………………………………….
5.7 Accountability ……………………………………………………………………………………………………………….
5.8 Contribution of this study ……………………………………………………………………………………………….
CHAPTER 6: CONCLUSION AND RECOMMENDATIONS ……………………………………………………………………
REFERENCES …………………………………………………………………………………………………………………………..
APPENDICES ……………………………………………………………………………………………………………………………
Appendix 1: Consent Form …………………………………………………………………………………………………..
Appendix 2: Information Letter …………………………………………………………………………………………….
Appendix 3: Information Sheet ……………………………………………………………………………………………..
ABSTRACT
The purpose of this study is to explore ex-prisoners’ perspectives on prison drug treatment in Ireland. Prison drug treatment has increased across Europe over the last 20 years both in availability and modality. However, the delivery of drug treatment services in a prison setting is not without its challenges. The prison population is a multiply disadvantaged group, which experiences a disproportionate level of health inequality and social exclusion. Substance misuse is prevalent for a high proportion of prisoners. This research is based on seven semi structured qualitative interviews with ex-prisoners who have had experience of prison drug treatment. The perspectives of ex-prisoners add important information to the sparse amount of literature available on prison drug treatment, especially from a user-perspective. The research found that different aspects of prison had a significant impact both on individuals and treatment. These aspects included the following: drugs in prison; prison environment; attitudes; and policies. An interesting feature of the study is the participants’ understanding of the many challenges faced by Irish Prison Service. One important finding is the need for more regular and up-to-date review of prison drug treatment. Accountability emerges as the most pressing need for prison drug treatment. While there are structures in place for complaints to be made, these structures are not fulfilling their function due to a lack of confidence in them. This leaves prisoners in a position of even greater vulnerability. In this study, ex-prisoners claim their voice amongst the voices of other actors in the field such as prison staff, medical staff, and politicians.
CHAPTER ONE: INTRODUCTION
1.1 Introduction
Prison drug treatment in Irish prisons raises many complex issues. There is a lack of research on it, with less research from a user-perspective. This research topic will focus on the perspective that ex-prisoners have of drug treatment in Irish prisons. Ex prisoners have had the experience of being in the prison system and the advantage of being able to reflect back on their experience. The proposed research hopes to uncover key insights which may help in identifying ways to improve drug treatment in prison, as well as recognizing what is working well. The research will be an opportunity for ex-prisoners to share their reflective learning from their experience and contribute to the discourse on drug treatment in Irish prisons.
1.2 Aim and Objectives
This research is an exploratory study of ex-prisoners experience of drug treatment in Irish prisons. The main objective will be to document, analyse, and apply the perspectives of ex prisoners concerning drug treatment in prison. Some areas of relevance will include the nature of drug use in prison; the prisoners’ experience of drug treatment; the effect that prison has on a person’s drug use; and reflections from a post-prison perspective. The contribution of ex prisoners will have an intrinsic value, along with having an important contribution to make towards the shaping of policy and practice. The research question is “what are ex-offenders’ perspectives on drug treatment in prison?”
1.3 Summary
The structure of this dissertation is described in this paragraph. Chapter One outlines the Aims, Objectives and the research question. Chapter Two considers the relevant literature. Chapter Three describes the methodology of the current study. Chapter Four outlines the findings of the research. Chapter Five discusses the implications of these findings. Finally, Chapter Six provides the conclusion and recommendations from this study.
CHAPTER TWO: LITERATURE REVIEW
2.1 Introduction
This chapter is divided into four sections. The first section considers the literature relevant to prison drug treatment in Europe, under the headings of participant profiles, the prison environment, delivery of prison drug treatment, and the types of prison drug treatment. The second section looks at prison drug treatment as a health strategy, taking into account health needs, human rights, equivalence of care, and duty of care. The third section examines prison drug treatment and its delivery in Ireland by looking at recent developments, from 1996 to present day. The fourth section highlights some specific challenges for prison drug treatment in Ireland.
2.2 Prison Drug Treatment in Europe
2.2.1 European context
Prison drug treatment is not exclusive to European prisons. There is information available internationally on prison drug treatment, mainly from Australia, Canada and the United States (EMCDDA, 2012). However, there is a lack of agreed international definitions on drug use, which makes discussion and comparisons difficult. The reasons for choosing Europe in this study are because of the similar understanding and approach to prison drug treatment in Europe. The European context also has information available on prison drug treatment through entities such as the European Committee for the Prevention of Torture and Inhuman or Degrading Treatment (CPT), and the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). While there are methodological differences between countries in Europe, regarding data collection and reporting, there is a greater coherence in Europe with regard to definitions and approaches to imprisonment.
2.2.2 Drugs in Prison
The European prison population has been estimated at 1.67 million people in 2013 (Aebi et al., 2015), with at least half of that population having a history of substance misuse (Stöver et al., 2014). According to Walmsley (2013), the European prison population continues to increase. In Europe, the prevalence of illicit drug use amongst the prisoner population is higher than the general population (EMCDDA, 2012). In their global prison population study, Dolan et al. (2015) found that HIV is higher amongst the prison population because of an over representation of people who inject drugs. McIlwraith et al. (2012) noted an increase in the use of benzodiazepines by prisoners who inject drugs. Wheatley (2007) explains that it is well established that there are high levels of drug use in the prisoner population. However, he explains that it is more difficult to establish the actual level of illicit drug use because of factors such as mandatory drug testing, which influences consumption patterns.
2.2.3 Efficacy of prison drug treatment
There is an acceptance among some commentators of the need to address substance misuse, not only in the general population, but also within the criminal justice system. In an examination of contemporary developments in the Scottish criminal justice system, Malloch et al. (2013) acknowledge the growth of drug treatment services while also cautioning against coercive treatment. In a survey of treatment programmes in 27 EU countries, Hamilton et al. (2014) observe a variety of treatment modalities and acknowledge their importance in addressing addiction issues among offenders. In a study of Finnish prisons, Obstbaum et al. (2015) recognise that evidence based practice for prison drug treatment had become the accepted standard in Finland. However, there is a lack of empirical evidence on how effective drug treatment is in prison. In a Scottish study on the impact of opioid substitution treatment on drug-related deaths after prison, Bird et al. (2015) found that opioid substitution treatment did not reduce early deaths after release. Stöver and Michels (2010) conducted a survey of studies on opioid substitution treatment in which they concluded that opioid substitution treatment was less effective in prison than in the general community. Though, in a systematic review and meta-analysis of European prison drug treatment, Koehler et al. (2014) establish the effectiveness of prison drug treatment in reducing future criminal activity, particularly through the use of substitution therapy; that paper examined in the region of 37,000 literature titles from six countries, with 3953 participants.
There is limited research on prison drug treatment in Europe (EMCDDA, 2012). Carpentier et al. (2012) acknowledge that the researching of drug related issues in European prisons is hampered by a lack of available data and varying methodologies. With even less research employing a user-perspective (Frank et al., 2015; Giertsen et al., 2015), the need for empirical research is acute.
Liebling and Maruna (2005, p. 13) identify prison addiction issues as an area where future researchers need to focus, as the lack of research, so far, has resulted in ‘sterility’ in this area.
2.2.4 Profile of Participants in Prison Drug Treatment
In Europe, individuals who take part in prison drug treatment share many similarities with their peers who engage with community based drug treatment (EMCDDA, 2012). Most of the information that is available on participants is deduced from qualitative studies (Vandam, 2009). Participants in prison drug treatment generally come from a background of disadvantage, which includes unemployment, lack of education, and unstable living arrangements (EMCDDA, 2012). These difficulties are often further compounded by childhood experiences of poverty, violence, and abuse (Swogger et al., 2011). Liebling et al. (2005, p. 216) describe these aspects as “imported vulnerabilities” which need to be managed in addition to the vulnerabilities which the prison environment itself generates. Bauman describes this concentration of vulnerable people as ‘prisonization’ where they, as the ‘underclass’, having already gone through a process of exclusion in society, now experience physical exclusion through imprisonment (1998, pp. 125-127). Bauman holds that ‘prisonization’ serves as a distraction from the real causes of insecurity in society (1998, p. 127). ‘Prisonization’ is a distraction because it misappropriates the blame for the causes of insecurity in society onto vulnerable people, which serves as a justification for their incarceration.
2.2.5 Prison Environment
The experience of drug treatment in prison is interlinked with the prison environment, which restricts movement and regulates life (Cohen and Taylor, 1972; Woodall, 2011; Stöver, 2014). Liebling and Maruna (2005) explain that the prison environment is, not only to do with the physical structure of walls and gates, but also includes the ‘hidden’ features of the social and affective dimension, which include fear, powerlessness, violence, and uncertainty. The motivations of an individual who participates in prison
drug treatment may not always be in line with the treatment goals. Motivations can be for different reasons such as, to attain privileges within the prison, to deal with boredom, to avoid violence from other prisoners, or to improve their health (EMCDDA, 2001; Crewe, 2006; Woodall 2011). Koester et al. (1999) calls this “self prescribed attempts at harm reduction” (1999, p. 1237). The decision of a person to begin a drug treatment programme is not an easy choice, whether in a community setting (Al-Tayyib et al., 2011) or a prison setting (Frank et al., 2015). While there are many reasons for participating in a programme, one dominant theme is the desire “to get a drug free and normal life after prison” (Frank et al., 2015, p. 159).
Prison is an environment in which some people stop using drugs, others begin using for the first time, while others change to a different substance because of availability (Vandam, 2009; Montanari et al., 2014). The reasons why prisoners use drugs in prison are diverse and include motives such as self-medication, as a coping mechanism, or as a distraction from routine (Boys et al., 2002; Crewe, 2006; Ritter et al., 2013; Baltieri, 2014). Prisoners who use drugs are in need of specific support because of their vulnerability, which includes poor mental health, a risk of overdose, and disadvantage coming from childhood experiences (Kothari et al., 2002; Swogger et al., 2011; Herbert et al., 2012).
Drug treatment programmes have a higher chance of success if they are relevant to the needs of the prisoner, take place over an appropriate period of time, and have the necessary “through-care” (Ramsay, 2003). If a prisoner can be open about themselves through drug treatment, in relation to their drug use and personal history, there is a greater chance of them changing and developing into taking greater responsibility for their life (Kolind et al., 2013). However, it can be difficult within a prison environment for prisoners to achieve this level of openness because of the risk involved in being vulnerable and the possibility of disclosing unreported criminal
offences (Frank et al., 2015).
2.2.6 Delivery of Prison Drug Treatment
In an evaluation of prison drug treatment from a user-perspective in Denmark, Kolind (2007) found that the manner in which drug treatment in prisons is delivered can be as important a factor as the content of the drug treatment programme itself. That evaluation included 37 semi-structured qualitative interviews with users. Those interviewed emphasised the importance of easy access to treatment, staff attitudes, and the availability of spaces. Similar studies from a user-perspective found that easy access to treatment was important and so too was the attitude of staff (Neale, 1998; Notley et al., 2012). Liebling et al. (2005) note how the manner in which a person is
treated in prison has a strong influence on perceptions of fairness and can strengthen or undermine the legitimacy of a prison.
Prison drug treatment in European prisons is generally carried out by prison staff. However, there is also input from community based groups and non-prison staff who have a relevant contribution to make. The delivery of prison drug treatment can raise conflicts of loyalty between staff and prison authorities. This can occur when the need for appropriate service delivery conflicts with the demands of the prison management for security and discipline (Pont et al., 2012; Elger et al., 2015). It is an ethical dilemma which indicates the complex nature of the role of staff involved in prison drug treatment (Council of Europe, 2006).
2.2.7 Types of Prison Drug Treatment in Europe
Drug treatment in European prisons varies from country to country. There is a spectrum of prison drug treatment. The services which are available across Europe vary in type and application. The services are detoxification, opioid substitution, counselling, educational and information programmes, and abstinence based programmes (EMCDDA, 2012). For many countries in Europe, detoxification is used as the standard response to opiate users and it varies in how it is prescribed in each country; for example, in Ireland, medical detoxification is available in all prisons, while in Turkey what is offered is information on drug addiction, on how to manage withdrawals, and on relaxation techniques (EMCDDA, 2012).
There is no one standard of prison drug treatment throughout Europe. Ireland provides both low and high threshold treatment. There are three broad approaches, as explained by EMCDDA (2012, p. 20).
• Low intensity drug treatment, which is short-term and includes counselling.
• Medium or high intensity drug-free treatment in prison within a drug-free setting.
• Medium or long term opioid substitution treatment, with methadone or buprenorphine.
Prison drug treatment aims to improve the health of participants and to reduce the use of illicit drug use in prisons. By investing in drug treatment in prison, there is a wider benefit for society such as crime reduction, an increase in public safety, and improved public health (Redondo et al., 1999; Kothari et al., 2002; Godfrey et al., 2004).
2.3 Prison Drug Treatment as a Health Strategy
2.3.1 Acute Health Needs
The Ottawa Charter (1986) acknowledges the impact that environmental influences or ‘settings’ have on the overall health of a person. This has led to prison being recognised as a ‘setting’ where health can be influenced (Woodall, 2011). In any case, prison gathers a specific population of people, who often have a poor relationship with health services outside of prison (Møller et al., 2007). Health needs of prisoners are more acute than the general population (Bridle et al., 2004; Barry et al., 2010), as indicated by the spread of diseases within prison such as Hepatitis C (Allwright et al., 2000), tuberculosis (Dara et al., 2015) and HIV (Stoever, 2002). This situation makes prison an important location for health promotion (MacNamara et al., 2014) and also for the implementation of drug treatment services (Long et al., 2004). However, Woodall (2011) point out that the prison environment is not only problematic for the implementation of the principles of health promotion, but that the prison environment undermines the key values of health promotion, which include participation, empowerment, and choice. While Garland has described prison as a ‘quarantine zone’
it is more for reasons of control rather than public health, where individuals who are seen as dangerous are isolated for the safety of the public (2001, p. 178). Garland has noted how prisons have become “a faute de mieux repository” for people with problems such as mental ill-health and substance misuse issues, among other things (2001, p. 178).
2.3.2 Fundamental Human Rights
Every human being has the fundamental right to the highest attainable standard of health. This right is articulated in Article 12 of the International Covenant on Economic, Social and Cultural Rights (United Nations, 1966). This right to health is shaped in practice by what is possible for the State to provide and, also, how, if at all, an individual engages that right (United Nations CESCR, 2000: No. 14). This fundamental right holds for prisoners as it does for the general population. The United Nations (1990) Basic Principles for the Treatment of Prisoners is clear that prisoners hold onto this right to health regardless of their imprisonment (Principle 9). The Council of Europe (2006) articulated that prisoners hold their human rights with the limitation of that which is lawfully restricted because of the requirements of incarceration.
2.3.3 Equivalence of Care
The principle of “equivalence of care” requires that people have access to a level of care that is equivalent to what is available to the general public in the same country (Niveau, 2007, p. 610). The principle of ‘equivalence of care’, as it relates to prison, is recognized on an international level in the United Nations Basic Principles for the Treatment of Prisoners (1990), the World Health Organisation (WHO) (Møller et al., 2007), and in the European and International Prison Rules. In Europe, the Council of Europe has recognized ‘equivalence of care’ as a basic principle for the care of prisoners (1993; 1998).
The principle of ‘equivalence of care’, when applied to prison, is a strong indicator of how society practices the principle of equality for all of its citizens (Niveau, 2007, p. 610). Equivalence is achieved when drug treatment services that are available in the wider community are also available and accessible to the same degree within the prison setting. However, it is acknowledged by WHO (Møller et al., 2014, p. 116) that equivalence of care in relation to drug treatment is not the case for many European prisons. This indicates a growing recognition of the need to reduce the gap between prison healthcare and community healthcare (EMCDDA, 2012).
2.3.4 Duty of Care
The ‘duty of care’ owed by the State to a prisoner requires that, not only is health care available, but that there are appropriate structures to promote well-being amongst prisoners and staff (CPT, 1998). The Council of Europe (1993) and the European Court of Human Rights (McGlinchey Case, 1999) have affirmed the ethical and organizational obligations of the State to care for the health of prisoners. The interpretation by the European Court of Human Rights of Article 3 of the European Convention on Human Rights (ECHR) established the special duties of authorities, not just towards prisoners with physical or mental disabilities, but also for prisoners with drug problems (Herrick, 2009).
While prisons are not the appropriate place for drug treatment, in the absence of an alternative, prisons need to respond to prisoners requiring drug treatment and do so in a way which respects minimum standards (Stöver et al., 2014).
2.4 Prison Drug Treatment in Ireland
2.4.1 Drug use in Irish prisons
The prison population in Ireland is a complex group of people who experience more acute levels of health inequality and social exclusion when compared to the general population (Barry et al., 2010; MacNamara et al., 2014). Drug use is a serious issue amongst prisoners in Ireland (Drummond et al., 2014). The Council of Europe noted that drug misuse (CPT, 2010) and drug availability (CPT, 2011) remain serious issues for Irish prisons and prison drug treatment. The lack of monitoring and oversight of prisoners in withdrawal and whether or not they were continuing to use illicit drugs while on methadone maintenance was also mentioned by the Council of Europe (CPT, 2011, p. 42). Appropriate support and in-cell sanitation for prisoners undergoing withdrawal was emphasised as a basic necessity (CPT, 2011).
Reports from the Inspector of Prisons (Limerick, 2011) and the Mountjoy Prison Visiting Committee Report (2012) also highlighted the drugs issue in prisons and indicated that most prisoners have addiction problems and that some people become addicted while in prison. The suffering of prisoners has been documented in Inspector of Prisons Reports as “inhumane and degrading treatment” (2010, paragraphs 9.2, 11.9 and 14.8). Cohen’s “states of mind” perhaps indicates a state of denial in Ireland as to some aspects of prisoner care where a “knowing and yet not knowing” state of denial exists (Cohen, 2001). However, the tolerance of illicit drugs in prisons may reflect an unstated containment strategy of prison staff so as to help prisoners cope with their environment and avoid escalation in prisoner violence. The tolerance of illicit drugs in prisons could also reflect a compassionate approach to dealing with prisoners. The supply of drugs into prisons would be significantly reduced if contact visits were prohibited. However, while reducing the amount of drugs in prisons, denying prisoners contact visits would also create significant distress for them and their families.
2.4.2 A Need for Research
The Irish Prison Service has been described as “a significant provider of drug addiction treatment” because of the high number of prisoners who have a substance misuse problem (NACD, 2006, p. xv; Comptroller and Auditor General, 2009, p. 68). Compared to the available research on drug use in Irish prisons (Allwright et al., 1999, 2000; Long et al., 2004; Dillon, 2001; Moore et al., 2007), Drummond et al. (2014) point out that there is very little on prison drug treatment in Ireland and even less from a user-perspective.
One criticism of the Report of the Steering Group on Prison Based Drug Treatment (2000) is that prisoners were not consulted in the process (Long et al., 2004). This shortcoming was remedied through the involvement of prisoners in the National Advisory Committee on Drugs and Alcohol Report (Drummond et al., 2014), which was part funded by the Irish Prison Service, with publication including a prisoner friendly Report.
The growth in prison drug treatment in Ireland over the last twenty years has not been reciprocated with a growth in research. While there is much research available on community based drug treatment, Drummond et al., (2014) acknowledge that there remains a deficit of research regarding prison drug treatment in Ireland.
2.4.3 A Recent History of Prison Drug Treatment in Ireland
Co-ordinated drug treatment in Irish prisons is a recent development beginning with the introduction of detoxification and addiction counselling in 1996. This was a response to the growing needs of prisoners in this area. In 1999, the draft Action Plan on Drug Misuse and Drug Treatment in Irish Prisons was published. This was a general strategy to develop prison drug treatment. It included expanding detoxification facilities and drug-free environments, providing methadone maintenance and hepatitis B vaccination, and providing addiction counselling and employment of registered nurses.
This was followed by the Report of the Steering Group on Prison Based Drug Treatment Services (2000) which sought to implement the Action Plan. It outlined a drug treatment service to be centralised in Mountjoy prison, which sought a multi agency approach and it recognized the principle of ‘equivalence of care’ which was
seen as “one of the most significant conclusions of the Report” (O’Mahony, 2002, p. 584).
A dominant theme of the Report is ‘through-care’ which seeks to develop and sustain continuity between the prisoner and community (O’Mahony, 2002). However, it has been criticized for not detailing what ‘through-care’ and ‘equivalence of care’ with the community would mean in practice (O’Mahony, 2002).
The Drugs Policy and Strategy of the Irish Prison Service was published in 2006 and is the main document of reference for prison drug treatment in Ireland. It points out the tensions that exist with the ‘twin challenges’ of security and the needs of the individual (2006, p. 2). It also acknowledges the reality of drugs in prisons and the wider effects that this can have, which include bullying, intimidation and violence. However, the Policy and Strategy sets out a zero tolerance to the presence of drugs, which is to be achieved through the elimination of supply, which the Inspector of Prisons has described as “an ambitious aspiration” (2009, p. 37). The Annual Report (2014) of the Irish Prison Service states that targeted cell searches including five targeted operations were carried out by the Operational Support Group. These searches resulted in a large haul of contraband being seized. The Report also states that four canine instructors were trained and are now available to deliver training to Irish Prison Service canine teams.
The Policy and Strategy aims to reduce demand for drugs in prison. It states that demand will be reduced in three ways (i) identify and engage with drug users, (ii) develop treatment options, and (iii) ensure that ‘throughcare’ takes place so as to support the treatment links between the prison and the prisoner’s community to which he or she will return to (2006, p. 13). ‘Throughcare’ is of particular importance to Irish (Lyons et al., 2010) and international (Strang, 2015) research which shows a significant risk of death upon release for drug using ex prisoners.
2.4.4 Delivery of Prison Drug Treatment in Ireland
There are 14 prisons in the State. The average daily population at the time of writing is around 3,650 prisoners (Irish Prison Service Website). Drug treatment varies between prisons, with both low and high threshold drug treatments. The Irish Prison Service has a Drug Treatment Clinical Policy (2008), the aim of which is to provide a high standard of care to prisoners with addiction issues. The Clinical Drug Treatment Policy gives evidence-based reasons for its recommendations. The recommendations are comprehensive and cover aspects of care such as methadone treatment guidelines, a confidentiality policy, detoxification guidelines, and much more. The most recent Annual Report (2014) of the Irish Prison Service indicates further development and enhancement of drug services. It also commits to reviewing the Clinical Drug Treatment Policy. The Annual Report also noted the ongoing development of drug free units in all closed prisons.
Central to the delivery of drug treatment services is courtesy and respect for everyone involved. In the recent Strategic Review of Penal Policy (2014), it was acknowledged that drug treatment does not work without an individual’s willingness to co-operate. However, the Mountjoy Visiting Committee suggested registering all prisoners affected by drug addiction in drug treatment programmes (2012). This suggestion, which has a coercive element to it, would need careful consideration. According to Seddon (2007) and Ryberg (2013), particular attention is needed to address the ethical, legal and moral difficulties raised by coercive drug treatment in prison.
Prison drug treatment in Ireland includes addiction counselling, methadone maintenance, medical detoxification, rehabilitation, information, and education programmes (Irish Prison Service Website). Individual assessment is seen as key to good service delivery (Clinical Drug Treatment Policy, 2008, p. 6). While there are questions as to the effectiveness of methadone maintenance, the Drug Treatment Clinical Policy accepts it to be more effective than having no treatment at all (2008, p. 9). While it should also involve psychosocial care (Stöver et al., 2014), on a recent visit from the Council of Europe, it was found that psychosocial support in this area was lacking in Irish prisons (CPT, 2011). Detoxification has been described by the Council of Europe (2002) as a gateway to treatment meaning that on its own, detoxification does very little to counteract long-term drug use (Clinical Drug Treatment Policy, 2008, p. 9, 22). However, after completing detoxification, individuals are required to receive other supports to ensure that their low tolerance does not lead to an overdose (Clausen, 2015).
Mandatory testing for drugs was introduced by the Irish Prison Service Drugs Policy and Strategy in 2006. It makes provision for the random selection and testing for drugs of between 5% to 10% of prisoners each month. Sanctions are imposed if a prisoner tests positive for drugs or refuses to be tested. Mandatory testing seeks to reduce demand for drugs in prison by engaging with drug-users so as to involve them in drug treatment services. Claims that mandatory drug testing encourages prisoners to switch from cannabis to heroin, because heroin exits the body quicker, have not been substantiated in research (Hucklesby et al., 2001).
Between 1999 and 2010, the Irish Prison Service has put over €8 million into healthcare services (Ailbhe Jordan, Medical Independent 10th June 2010). According to the Annual Report (2014), the budget for the Irish Prison Service is €334.188 million. This is slightly down on the budget for 2011 which was €347.583. There was no figure available for spending on prison drug treatment in the 2014 Annual Report. Therefore, it is not possible in this study to make comparisons with other expenditure in the Irish Prison Service. Most recently, the Irish Prison Service has introduced the Prisons Pilot Project Helpline which began in December 22nd, 2014. It is a Helpline from which prisoners can discuss issues including drugs and alcohol, with no time limit, and in confidence. It is an innovative approach to supporting prisoners. As the Prisons Pilot Project Helpline will be reviewed in 2015, there could be relevant information available to guide the Irish Prison Service, taking into consideration the confidentiality of the service.
The challenges for prison drug treatment in Ireland are multifaceted and complex. However, this also presents an opportunity for positive intervention through drug treatment programmes (Moore et al., 2004) particularly when a prisoner wishes to address drug misuse (Long et al., 2004).
2.5 Some Challenges for Prison Drug Treatment in Ireland
2.5.1 Need for Accountability and Review
Coyle notes the consequence of treating the prisoner as an object rather than a person (Liebling and Maruna, 2005). In such cases, the role of the prisoner is to simply co operate with decisions made by others without being involved in the decision themselves. However, accountability requires that those who make decisions about others are also answerable for those decisions (Cavadino and Dignan, 2007, p. 230). Rogan (2014, p. 3) comments that “perhaps the most fundamental difficulty in the Irish prison system concerns the weakness of structure for ensuring accountability for decisions taken by the prison authorities or responding to matters of concern.” It is evident from the development of prison drug treatment in Ireland that prison conditions have improved. However, there are issues of concern within prison drug treatment that would benefit from a strong, independent system of oversight.
Cavadino and Dignan (2007, p. 230) note that a number of agencies concerned with prisons can elicit “a degree of answerability” for the decisions made in prisons. The office of the Inspector of Prisons has been an important development in the area of accountability, by highlighting shortcomings related to prison drug treatment. Other forms of accountability include legislation, Annual Reports, Visiting Committee Reports, International Committees Reports and independent oversight such as from the Irish Penal Reform Trust. However, the prison, as a closed environment, makes it more difficult to establish accountability (Harding, 2007).
A review of drug treatment in prison was recommended by Mountjoy Visiting Committee (2012). On 18th May 2015, at the launch of the Joint Probation Service Irish Prison Service Strategy 2015-2017, the Minister for Justice acknowledged the importance of improved addiction services for offenders. The Minister then announced that a Review of Drugs and Alcohol Services to Offenders would begin in the near future. There are no more details available on this Review.
2.5.2 Unreliable Access
While there is a high uptake of drug treatment in Irish prisons, within the range of 70 90% of those interviewed by Drummond (2014), access to treatment is not always available (Drummond et al., 2014, p. 88). The high level of engagement by prisoners is seen as a strong indicator that the prison setting is an appropriate place for drug
treatment (Drummond, 2014). However, the difficulty with access to treatment leads to frustration amongst prison staff and prisoners (O’Gráda, 2010). The Inspector of Prisons in Ireland highlighted the impact that 23 hour lockdown has on limiting the access to drug treatment for that prisoner category (2013, p. 13). It also undermines
the prison drug treatment system by inhibiting access to treatment. The access difficulty appears to be a continuing issue, as it was raised recently as a concern by the Strategic Review of Penal Policy (2014). Other challenges which interfere with full access to treatment include the prison regime, staff attitudes, and the relationship between staff and prisoners (McIntosh & Saville, 2006).
2.5.3 Effectiveness of prison drug treatment
The 2006 Policy and Strategy acknowledges the importance of having good quality research to underpin its approach (2006). It acknowledges the need for more research into prison drug-related issues. In the context of the Policy and Strategy, there is meant to be research on drug misuse in prisons, an evaluation of programmes and interventions and a sharing of research data. The Policy and Strategy also aims to evaluate the effectiveness of drug interventions.
The effectiveness of prison drug treatment will be very difficult to evaluate without sufficient research. Research is important to influence the decision-making of policy makers and service providers. This research needs to be kept up-to-date and done regularly and not just focused on the elimination of drug use. Recent international
research (Hamilton et al., 2014) pointed out shortcomings between routine practice and international research, which indicates the need to ensure that evaluation of routine practice is a regular occurrence. Liebling and Maruna (2005, p. 2) note that shortage of research on the modern prison has generated “an ethical and intellectual void” in which the result has been the undermining of the quality and legitimacy of prisons.
2.6 Ireland in the context
Comparisons between Ireland and other European countries are made difficult because of the variations throughout Europe in data collection and methodologies. While there is consensus in most European countries of the need for a developed prison drug treatment service, a European classification system would assist in the collection of relevant data and assist in the development of current, evidence-based information.
Opioid substitution is one of the main treatments in most European countries. Comparisons are difficult to make because of the absence of reliable data as to the number of prisoners using this treatment. With regard to the long-term care of prisoners, compared to Greece, Cyprus, Lithuania and Slovakia, where long-term opioid substitution is not prescribed, Ireland compares favourably by providing long term opioid substation.
While there is interagency work between the Irish Prison Service and health care providers for the delivery of prison drug treatment in Ireland, there is a trend in Spain, France, Italy, Slovenia, Sweden, United Kingdom and Norway to transfer responsibility for the delivery of health care, which includes prison drug treatment, to the same structure which provides healthcare in the community (EMCDDA, 2012). This shift affects 40% of the European prison population. It is a response to the need for integration of prison health structures with those in the community and to improve the continuity of care for prisoners. In Sweden and the United Kingdom, there was
also increased funding to encourage prisoners to engage with drug treatment (EMCDDA, 2012). Given that Spain, Scotland, and Italy are considered as operating within best practice for both harm reduction and treatment services, and are also part of this trend of integration, it is an opportune time to consider how Ireland may respond to this trend.
2.7 Conclusion
A constant refrain throughout this literature review has been the lack of empirical research in general on prison drug treatment and in particular from a user-perspective. This chapter has considered prison drug treatment, in general, in both a European and Irish context, with a particular focus on the service user. While there are many standards and legal requirements in place and many issues needing attention, what arises from this chapter is the need for robust structures for accountability and regular, up-to-date research. While the perspective of ex-prisoners is not the final word on prison drug treatment, it does contribute an authoritative narrative which has a solid contribution to make towards the design, delivery and administering of an ethically sound prison drug treatment service.
CHAPTER THREE: METHODOLOGY
3.1 Introduction
This chapter identifies and discusses the methodological framework employed in this study. It contains an overview of the research rationale, strategy, design and approach. It outlines the relevant information regarding participants. The data collection and analysis is discussed. Finally, the ethical issues and limitations of the research are considered.
3.2 Overview of the Research Rationale,Strategy, Design and Approach
The aim of this research is an exploratory study of ex-prisoners perspectives of drug treatment in Irish prisons. It does not purport to be a comprehensive examination. The research question is “what are ex-prisoners perspectives on drug treatment in prison?” The main objective will be to document the perspectives of ex-prisoners concerning drug treatment in prison. Some areas of investigation will include the nature of drug use and drug treatment in prison; the prison environment; the prisoner’s experience of drug treatment; the effect that prison has on a person’s drug use; and reflections from a post-prison perspective. The contribution of ex-prisoners will have an intrinsic value, along with having an important contribution to make towards the shaping of policy and practice.
The research design is phenomenological and the research has a qualitative approach. This allows for the insights of those interviewed to be expressed through understanding the subjective experience of the ex-prisoner of drug treatment in prison (Gelo et al., 2008; Foddy, 1993). As there is little research available on drug treatment in Irish prisons, an exploratory study will shape the qualitative strategy (Stebbins, 2001, p. 6). With this gap in research, the qualitative research approach needs to be of a depth and quality to offer a substantial body of knowledge. A qualitative approach uncovers attitudes, perceptions and understandings and looks into the meaning of what is presented (Burnett, 2009). This is distinct from a quantitative approach which measures and weighs information from a more objective disposition. The qualitative approach compliments the phenomenological research strategy which acknowledges the knowledge and understanding contained within the lived experience of participants (Creswell, 2011). The qualitative approach and phenomenological strategy will help uncover how people make sense of their lives in their own words and, so, enable an understanding of the context of drug treatment in prison (Lincoln et al., 2003, p. 603). The importance of the subjective view of ex-prisoners in this research is an ‘interpretivisit’ epistemology. This means that the topic is viewed through the
perspective of the participant (Bryman, 2012). To compliment this, the research uses a ‘constructionist’ ontology which understands the world as “constructed in and through interaction” rather than through external definitions (Bryman, 2012, p. 34). This will be of particular relevance when noting the official reasons given for why people engage with prison drug treatment.
compared to the reasons given by individuals themselves as to why they engage with prison drug treatment.
3.3 Research participants
At its core, this research seeks to understand drug treatment in Irish prisons from the perspective of the ex prisoner and to understand the lived experienced and meaning of daily life. It is an exploratory study which uses a convenient sample and scopes out areas for further research. Therefore, the sample selected is not a representative sample. There were four criteria for inclusion of participants. These were to be an ex prisoner, who had used drugs and/or alcohol, who was over eighteen years of age, and had some experience of prison drug treatment. Though initially the researcher set out to talk with anyone within that criteria, it was only men who presented for interview. In addition to the inclusion criteria, participants for this research, had to have spent at least one month in prison, either on remand or under sentence. The periods in prison of participants who were interviewed ranges from nine months to 12 years. The participants had used alcohol and a range of drugs including heroin, cannabis, amphetamines and cocaine.
There are difficulties in accessing ex-prisoners for different reasons. These include issues of bias, trust, and labelling. In light of these obstacles, and the need to progress the research, non-probable purposive sampling was used (Denscombe, 2010a). This meant that the selection of participants was influenced by those who were available and willing to participate and who fulfilled the criteria (Rubin and Rubin, 2005). As the sample selection was not representative of the group, the fact that it is small in number does not interfere with the research objectives. The researcher considered using focus groups but decided against it because of the possibility of people being uncomfortable to speak freely within a group. The main advantage in using focus groups would have been expediency. The researcher found that individual interviews, with the sample selection of 7 participants, was time-consuming.
Reflexivity is an important consideration for the role of the researcher. It acknowledges that there is a relationship between the researcher and the social world being studied (Punch, 2005). Reflexivity means that a researcher cannot attain a purely objective standpoint outside of the social world but uses their perspective of the world to make sense of it.
3.4 Data Collection and Procedures involved
A qualitative research approach was used to collect data. This was carried out through interviews with participants which assisted in unpacking the complexity of drug treatment in prison (Creswell, 2009). The method of data collection was structured through the in-depth interviews of seven adult males. This approach helped establish a deeper understanding and portrayal of the perspectives of people who have spent at least one month in prison and who have had some experience of drug treatment in prison (Denscombe, 2010; Creswell, 1994). The researcher has particular experience of working in a prison. Costley et al. (2010) hold that work-based knowledge can be an advantage because it provides a knowledge and experience gained from that work. Initial contact was made through the director of five community based organisations which work with ex-prisoners with the Information Letter (Appendix 2). For unknown reasons, there was no response from two of the organisations. Out of the three organisations who responded, two were available to participate within the given time frame. Issues of access, gatekeeping, and informed consent were considered. To receive informed consent from a participant requires a clear and informative Information Sheet (Sarantakos, 2005). The Information Sheet (Appendix 3) which was used for this research explained what the research was about and why it was being done. It also explained the time commitment required of the participant, which was one interview for a maximum period of one hour. The interviewee was asked if it was acceptable to record the conversation. Three participants did not give permission for the interview to be recorded. In those cases, the research took extensive notes during the interview and for two hours after each interview. The reasons given for not having interviews recorded were to do with doubts about confidentiality, the similarity to being interviewed at a Garda station, and not wanting to get in trouble. The interviewee was informed before the interview began that he was free to discontinue the interview at any time. Confidentiality and its limits were explained and the consent form (Appendix 1) was signed. After each interview, reference to the person’s name on the digital recorder was removed and replaced with a number to protect anonymity. Once the interview was transcribed and verified, the interview was deleted from the digital recorder.
Participants were not approached directly by the researcher. Instead, an information letter (Appendix 2) was emailed to the director of each project seeking access to research participants. The director acted as an initial gatekeeper, deciding whether the request should be granted and they appointed a staff member to continue the process. The staff member, appointed as a gatekeeper, facilitated access to the project, helped locate research participants, and identified a suitable place for the interview to take place. Compromise and negotiation were part of the process to seek access. This helped to establish good boundaries and mutual understanding. It was important that the seven participants had a history of drug and/or alcohol use before or during their prison experience. The lived experience of those interviewed brought about a better understanding of the research topic (Creswell, 1994). A qualitative approach helped draw out the meaning and context of the lives of people interviewed. This gave a solid foundation on which to investigate and scope out the research topic.
3.4.1 Interviews
All the interviews took place in the Project where the individual was contacted, except for one which took place in a hotel board-room. The reason for the hotel interview was because the participant wanted more privacy than what was possible in the Project. The researcher suggested a hotel board-room and the participant agreed. The
researcher paid for the hire of the room. All the interviews had a conversational style rather than formal. However, it is important to note that, while conversation and interviews have similarities, there are important differences (Denscombe, 2010b). Some of these differences are that consent is required from the interviewee and that the agenda is set by the researcher (Denscombe, 2010b).
The interviews in which a digital recorder was used helped the researcher to focus more on the participant. It was also very beneficial in transcribing the interview afterwards. The use of a digital recorder avoided the distraction of note taking and also helped to know what exactly was said. Some notes were taken during the recorded interviews to capture body language and other things that a recording would miss out on.
It was important that the main questions were defined enough so as to have a specific focus but not so defined that it would pre-determine responses (Rubin and Rubin, 2005). To encourage participants to talk more and to avoid a flood of questions from the researcher, there were 27 questions in the interview schedule. This was to avoid rushing through an interview and also to give the participant an opportunity to talk (Rubin and Rubin, 2005). The interview schedule was reviewed after the first interview. This review resulted in some questions being eliminated because they were ‘closed’ questions which inhibited the flow of the interview. Other questions were eliminated because the researcher felt that they encroached on the interviewee’s privacy. Other questions were merged into one because of similarities.
The questions for the interview began with general questions about socio demographics and drug-use history. As the interviews continued, there was more specific information sought, such as the type of drugs used, frequency of use, and perceptions of drug treatment in prison (Denscombe, 2010a). Literacy difficulties were taken into consideration so that the interview language was presented in plain English and easy to understand. As the interview process was an essential part of the research, it needed to be organized properly beforehand so that the interviewer was familiar with the flow of questions. The interviews were purposeful and controlled by the interviewer so that it did not stray into irrelevant areas (Kvale, 1996). There was a struggle at times between the researcher and the interviewee to keep the interview focused on prison drug treatment. This was because when interviewees became comfortable they were inclined to continually talk.
3.5 Framework for Data Analysis
Data analysis was inductive. The qualitative researcher used the data as the foundation on which to the apply theory and concepts. The data was thematically analysed manually. Each interviewee was given a unique number so as to help with easy access back and forth over the data. It also provided anonymity for the participants. Important themes and concepts in the transcript were coded and these items became apparent after familiarity of the transcript was achieved. Every code was linked to each other in an overall coding structure (Rubin and Rubin, 2005). An integrated approach for coding was used to include a predetermined set of codes and a set of codes that arose from the transcript. Some codes were obvious because they were explicitly mentioned in the text, while other codes were less obvious but were still noted. There were particular phrases, like motifs, throughout the text, which gave insight. Definitions were important so as to properly assign themes, concept and issues. Being clear on definitions and context helped to clarify how items should be coded. By grouping certain things together, a picture began to emerge of what was being analysed. This was compared and contrasted with findings from other research so as to come to a better understanding of the research topic. Coding produced a picture of themes and contexts which then provided a platform from which to present findings. Themes should have numerous quotations and perspectives to flesh them out (Creswell, 2009, p. 189). This helps with the thematic analysis (Bryman, 2012). The repetition of a topic, however, does not automatically make it a theme. Rather, a theme develops through reflection.
As the coding was produced, new ideas emerged, requiring a number of reviews and changes before the final code was decided on. How the researcher shaped the coding had definite impact on the results of the data analysis. Therefore, it was important to give sufficient attention to this important process. Coding helped identify similarities and differences between different codes and also how different people experienced a particular event (Rubin and Rubin, 2005).
3.6 Ethical Issues and confidentiality
Ethics is an essential consideration for all social research (Punch, 2005). It is
important because social research concerns the personal lives of people. This needed
to be handled appropriately, with the added effect of the participants in this research
being a vulnerable group. Ethics guards and protects the integrity of the research
project (Thorseth, 2003). It also protects the good name of research, enabling future
research to be carried out, so leaving a legacy (King, 2000). In this research, there are
ethical issues raised regarding personal disclosures, access to participants, storing data,
and informed consent (Israel et al., 2006). These ethical issues were navigated under
the ethical guidelines for taught postgraduate research dissertations at DIT. The
methodology is aligned with these guidelines. Ethical approval was provided by the
Head of School of Languages, Law and Social Science in DIT.
Confidentiality was assured, with the exception of any disclosure which indicated a
danger to the participant or to someone else. Access to participants was through
gatekeepers.
Each Project was furnished with a Letter and Information Sheet
explaining the research. Each participant received a Letter and Information sheet.
Informed consent was sought from participants through the provision of an information
sheet with any necessary explanation. Data from the study was stored securely during
the research and then destroyed when the research was completed.
3.7 Limitations
The present study was subject to a number of limitations. Firstly, the group of participants is small in number. It will not be possible to make generalisations from such a small group (Bryman, 2012). While it is not possible to hold complete objectivity (Bryman, 2012), the use of an ethical and professional approach to this research helped to overcome this limitation. Another limitation is that all of the participants were men. A gender balance may have had an influence on the results. With these limitations, the sample is not representative of the whole prison population nor of users of prison drug treatment.
While the researcher has past experience of working in prison, the work was not specifically related to prison drug treatment. However, it nonetheless bestows on the researcher an appreciation of the prison environment. This familiarity is beneficial in providing a ready-made foundation on which to build on but it may also be a drawback by placing the researcher too close to the research topic for objectivity. However, the substantial literature review provides considerable material for a challenging exchange on any research findings (Denscombe, 2010a).
3.8 Conclusion
This chapter has identified and explained the methodology under which this research will be carried out. It has also explained why and how qualitative data collection were used so as to help achieve the aims and objectives of this research. The framework for data analysis gives the process by which the information will be analysed. The ethical issues raise awareness about the importance of observing best practise for the protection of everyone and especially the participant. Finally, the limitations of this research were mentioned.
CHAPTER FOUR: FINDINGS
4.1 Introduction
This chapter presents the data which was gathered through the interviewing of seven participants. The profile of the participants and the selection criteria is outlined. The data is divided thematically into six themes. The six themes are the prison environment, prison drug treatment, communication, change and Policy impact, attitude and motivation, and, finally, accountability. Each theme is expanded on with the aid of the narrative from participant interviews.
4.2 Profile of Participants
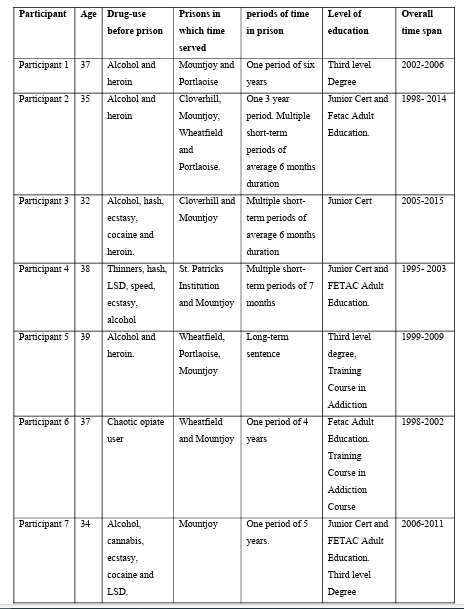
Seven Irish white male participants were interviewed individually on one occasion for a period of between 25 minutes and one hour. Each participant fulfilled the selection criteria for the research. This criteria was that each participant was over 18 years of age, who had used drugs and/or alcohol and had some experience of Prison Drug Treatment in Ireland. The use of an audio-tape was permitted by four of the participants, with the interviewer taking notes for three other participants. The reasons for not wanting to be audio-recorded were that they did not want the audio tapes to get them into trouble; audio-recording reminded participants of Garda interview rooms and the Boston College IRA Tapes were an example of how research agreements on confidentiality can be broken.
At the time of interview, four participants were in full-time employment and three were participating in services which seek to re-integrate ex-prisoners into society. The first experience of prison for participants was between the ages of 18 and 24. The overall time span relating to prison ranges from 1995 to 2015. This gives a good time line with regard to the development of prison drug treatment over a twenty year period. Interviewees articulate a wide range of perspective on prison drug treatment. Interviewees are noticeably insightful, reflective, and balanced in their comments. Being at a stage in life where they can reflect back on their prison experience, their perspectives are enriched by their age, education, work experience and life experience.

4.3 The Prison Environment
The first theme presented is the prison environment. It arose as a theme out of a general question posed to participants of what they found difficult about prison drug treatment. It was a broad question so as to encourage participants to talk about their experience of prison drug treatment. As participants responded to the question, they introduced specific aspects of the prison environment which impacted on their experience of prison drug treatment. These aspects of the prison environment were considered as normative. Some aspects were clearly experienced as negative or positive in their effect. There are five aspects to the prison environment presented below.
4.3.1 Prison Culture
Prison culture, as it relates to prison drug treatment, arose in all of the interviews. Prison culture is often marked with a constant threat or perceived threat to personal safety which can hold individuals in a state of hyper vigilance. For one participant, he did not experience prison drug treatment in itself as particularly difficult. However, the prison environment had an adverse effect on his willingness to engage fully with prison drug treatment.
“What would be difficult is you are in an environment, a prison environment. So its quite difficult … to show any vulnerability” (Participant 6, Age 37)
The threat of being attacked in prison meant that there was a constant fear for one’s personal safety. As a result, individuals developed a suspicion of their surroundings. Prisoners sought to maintain their full physical strength in case of attack. Therefore, participating in prison drug treatment was perceived as leaving you in a weaker state and so more vulnerable to attack.
“Prison is a rough place … if you’ve to watch your back all the time and then you take treatment, it leaves you weak.” (Participant 2, Age 35)
This participant believed that the prison setting was not suitable for drug treatment. He pointed out that drug treatment is not just about ‘getting clean’. It also involves psycho-social aspects such as a stable environment and absence of threats.
“Prison isn’t the place for that (drug treatment). It’s not just about getting clean, you need a steady life but in prison you’ve gotta watch your back, you’ve gotta survive … doing treatment in prison leaves you weak to attack”.
(Participant 3, Age 32)
4.3.2 The Prisoner Code
The ‚Prisoner Code’ is a value system amongst prisoners which demands loyalty to fellow prisoners. It is an unwritten but clearly understood prohibition on reporting or ‘ratting’ to prison authorities. One participant spoke of how an individual in his therapy group was using drugs. As the ‘prisoner code’ demands strict loyalty to other prisoners, he felt unable to challenge that individual in front of the therapist and prison staff. Therefore, the ‘prisoner code’, which is an inherent part of the prison environment, had compromised the therapy group. “No matter how big you are or how tough you are, if you are on a treatment programme and there’s somebody who’s using, you’re not gonna call it. It’s against the Code” (Participant 6, Age 37)
4.3.3 Availability of drugs
The Drugs Policy and Strategy (2006) of the Irish Prison Service strives for a drug-free prison environment. The reality, though, is that drugs and alcohol are available in Irish prisons. The availability of drugs in prison presents a constant difficulty to people who are trying to achieve or maintain a drug-free existence. The effect on the prison environment is that there is increased tension and the integrity of the drug treatment programme is undermined, as this participant explains.
“If you are doing the drug treatment programme and if you have two people in it who are getting drugs on their visits, that’s extremely difficult and then you are going into meetings or groups and talking bullshit. You’re there and you have to listen to that and you know they are using”.
(Participant 6, Age 37)
4.3.4 Prison as an initiation into drug use
The prevalence of drugs in prison is one of the many challenges which the prison environment presents to prisoners. While a high number of prisoners enter prison with an addiction issue, there are some individuals for whom prison is where they are first introduced to heroin. One reason for using drugs in prison is as a way to cope with the prison environment.
“You’d have lads from the country being introduced to that (drugs). They didn’t have a chance. Some of them would have taken heroin for the first time when they were in prison. Could you blame them? They needed to survive. They needed something to keep them sane and get them through the day”.
(Participant 5, Age 39).
4.3.5 Benefits of the Prison Environment and Drug Treatment
Having detailed the negative aspects of the prison environment, participants were able to identify positive aspects of the prison environment. One participant demonstrated how it was possible for him to become drug-free in prison. He also realized that it was a significant achievement.
“The longest drug free time for me was 12 months. That’s a big deal when you think about it, to be clean for a whole year.” (Participant 5, Age 39)
Certain areas in prison were considered to be more supportive of an individual engaged in prison drug treatment. These areas within the prison environment deliberately supported a drug-free life. One participant appreciated the increased contact he had with family and the opportunity to study for a degree.
“I was at the stage where I wanted to get to ‘enhanced’. The conditions were good there with more phonecalls, gym, teachers, extra visits … I did an Open University degree at the time but not through Mountjoy. I stayed on the enhanced wing in St. Pats. I’d sleep there in Pats and then do my studies and go back to St. Pats.”
(Participant 5, Age 39)
One specific benefit of being in a drug-free environment is that it provided a space for self-reflection.
“It was time to think straight. I watched a lot of what was going on. Stuff I was missing when I was using. But I learned a lot by watching.” (Participant 5, Age 39)
4.4 Prison Drug Treatment
The second theme is prison drug treatment. It was a strong theme throughout all of the interviews. This is not surprising due to the focus of the research. Participants raised specific areas of prison drug treatment and commented on them from their perspective. As participants were in prison at different times, between 1995 and 2015, there are different views on prison drug treatment, depending on when the participant was in prison. This difference in view is for the most part because of changes in prison drug treatment between 1995 and 2015.
4.4.1 Person-centred treatment
One of the participants who had recent experience of prison between 2005 and 2015 felt that a person-centred approach to prison drug treatment was very important. In his case, he felt unable to make informed decisions on his own treatment because of inflexibility in the delivery of prison drug treatment and competing priorities within the prison, such as security.
“It’s their way or no way. Treatment is way down the list of what’s important. That’s just the way it is. Take it or leave it”. (Participant 3, Age 32)
4.4.2 Methadone
There was a strong reaction against methadone maintenance amongst some of the participants. For them, methadone maintenance had a negative connotation and its use was to be avoided. Methadone maintenance was perceived as ineffective in helping the person to change and was an obstacle to recovery.
“I purposely didn’t want to be on methadone ‘cos I’ve seen what happens. Yous get out the same way as you get in” (Participant 1, Age 37)
Another participant viewed methadone maintenance as a life-long imposition and he distanced himself from people who are on methadone maintenance.
“Methadone, yeah? No way pal and have me stuck on it forever. I see plenty of those around. I’m not one of them. You go on that shit and you’re on it forever mate. You never get off it”. (Participant 3, Age 32)
4.4.3 Stigma
Even though drug and alcohol use is part of daily life in prison, stigmatization could occur. One participant recalled a time when individuals who were publicly identified in front of other prisoners as being involved in treatment were asked for information on AA meetings.
“In the main jail it was hassle for the prison officers to come out to the yard … and there was also a stigma ‘cos you were getting called in the yard out of 300 prisoners and asked if there’s an AA meeting on” (Participant 3, Age 32)
4.4.4 Staff
Medical staff were seen in a generally positive light, as mentioned by this individual.
“The medical staff are super. They detox you down 5 mils each time. I was worried I wouldn’t sleep. So I got a sleeper too”. (Participant 2, Age 35)
However, some prison doctors were viewed as overly cautious and controlling. In the medical context, the prisoner seemed at times to be a passive receiver of treatment without much input into decision-making. There was some awareness from this participant of the dangers of detoxification.
“The prison doctor … is very cautious and very sceptical of people reducing off methadone … they take a real kind of attitude to people when they come down off it because they see the other side of it because when you come down off it and use heroin there’s a chance you could relapse … it feels like control … there’s always caution instead of encouragement … when people are trying to come down off methadone” (Participant 7, Age 34) For one participant, the confidentiality between doctor-patient was encroached upon for reasons that seemed to be about curtailing drug supply.
“You’d have a prison officer behind you when you’d meet a doctor and that wasn’t good…If I met with a psychiatrist I’d have a private meeting but not with the doctor…I guess it’s because you’d have lads looking for tablets.” (Participant 5, Age 39)
This participant was able to recognise that the courtesy and respect between staff and prisoners was a two-way process.
“I found the drug treatment programme and the Training Unit for me hugely beneficial … I suppose the prison will work with you as long as you’re working with them … If you are going in and calling prison officers scum bags and pigs, they’re human beings, they’re not going to help you”. (Participant 6, Age 37)
4.4.5 Drug Treatment Programme
The Drug Treatment Programme, at times, was experienced as being somewhat contrived. This participant explained how the selection seemed to be random and lacking a thorough preparation. A more gradual preparation process would perhaps have benefited his group.
“I would have got the sense it (prison drug treatment) was superficial. You had eight people in on a landing and …. There’s no kind of going through the process of change …. like, one day you are an addict in the main jail … where … anything goes to going into therapy the next day with people you never met
before”. (Participant 6, Age 37)
The same participant continued his reflection on prison drug treatment by considering the inter-personal dynamics of individuals in the group. These dynamics had an impact which could help a group develop or prevent a group from functioning.
“If you get one or two bad eggs and they have an influence they can ruin it for everybody. And as much as the other people might want it, you’re stuck with that group of people. So that has a huge influence on how you do”. (Participant 6, Age 37)
4.4.6 Fellowship Meetings
Fellowship Meetings were mentioned regularly by all interviewees as being very important.
“I used alcoholics anonymous [AA], they came into the prison.” (Participant 7, Age 34)
“The NA [Narcotics Anonymous] meetings were great. There was no other place like them”.
(Participant 2, Age 35)
The consumption of alcohol was generally a seasonal occurrence, particularly at Christmas time. However, it was explained that alcohol was consumed on a more regular basis by foreign nationals. While Fellowship meetings were available, they were times at times irregular.
“Alcohol … its more of a cultural thing. The foreign nationals take a lot of it … but there were lads who had a drink problem … there were Fellowship meetings like AA and NA so that would have helped. But they were in trends
and at time sporadic”. (Participant 5, Age 39)
When it was not possible to have a Fellowship meeting organized officially, prisoners showed initiative and organized their own.
“There was no regular access by NA so we self-organised and arranged a time and place every week” (Participant 5, Age 39)
4.4.7 Access
Access to prison drug treatment was experienced as difficult at times and seen as the biggest issue for prison drug treatment. Lack of access was due to different reasons but mainly because of the limited number of spaces.
“Now (2015) the biggest issue is getting access … there are only 9 places on it … the prison population is 3400 … on average 70% will have addiction issues. Do the sums on it per year …. that’s a total of 54 lads per year. But that’s if all 35 goes well and they complete the course … it’s not big enough yet” (Participant 5, Age 39)
Access could also be hampered because the motivations of some participants were at odds with what was required for prison drug treatment. This could have the collateral effect of denying genuine participants access.
“The officers might not let you through … part of it is we were all tarred with the same brush. You could have lads who were serious about getting clean and then you’d have others who had a different plan … pass information, get at someone.” (Participant 5, Age 39)
4.5 Communication
The third theme is communication. This theme arose from questions to participants about how they got to know about prison drug treatment. The responses from participants suggested a communication gap between service providers and prisoners. Participants describe different time periods between 1995 and 2015. An indication of the period being referred to is included where available.
4.5.1 Lack of Communication
Participants indicated an overall lack of communication from prison authorities regarding prison drug treatment. This resulted in a number of participants becoming passive recipients of treatment, with very little active participation. One participant recalled that, in 1995, there was no systematic screening process for prison drug treatment. His experience of prison drug treatment was random and lacked co-ordination.
“I would have just gone 18 (1995) … the Guards, em, just opened the door and asked who was to see the doctor. That was it. That was the only question … I got 50mils of brown methadone, having … only smoked heroin once at that stage” (Participant 4, Age 38)
Communication improved somewhat between 1998 and 2002. During this time, period official communication regarding prison drug treatment was actively distributed amongst the prison population.
“it (prison drug treatment) would have been advertised in the prison … I don’t know what it’s like now but at the time they used put flyers around” (Participant 6, Age 37)
Some communication issues were solved by prisoners sharing information with each other through word of mouth.
“You heard about the meetings. It was somewhere to go. My first experience of drug treatment was NA … I thought about me problems a lot” (Participant 2, Age 35)
But, in general, those interviewed were unaware of supports.
“I wasn’t aware of any supports. When I was on remand I hadn’t a clue what was available”. (Participant 5, Age 39)
4.5.2 Negative consequences
One danger resulting from the lack of communication was made evident by this participant’s experience of going into withdrawals. His experience is from 2005.
“No I wasn’t told about treatment. Soon after I went ‘cold turkey’ … I was shaky, puked for a day and a half, panic attacks. The rattle was bad. I was in pieces after it. I got clean for 6 months until I was let out again. But then you’re in and out again, you know, the revolving door … and it’s the same shit all over again”.
(Participant 3, Age 32)
4.5.3 Importance of Effective Communication
Participants in general were able to appreciate the multi-dimensional composition of prison, with its many demands and pressures on resources. However, participants expressed disappointment at not being informed by prison authorities about situations which had a serious impact on them. One participant gave the example of finding it difficult to access a doctor. In hindsight, the participant understands the complexity of healthcare in prison. However, he also explains that better communication would have helped him understand why access to a doctor was difficult.
“At that time doctors were difficult to access … I understand now that it was complex. There was more to the picture than what I wanted. I didn’t understand then that detoxification could be dangerous and that doctors were slow because of that … it might have helped if it was explained”. (Participant 5, Age 39)
4.6 Change and the Impact of Policies on Prison Drug Treatment
The fourth theme is change and the impact of policies on prison drug treatment. Those interviewed for this research project experienced prison in Ireland at different times between 1995 and 2015. Throughout the interviews, there are indicators of change over that time period which have shaped prison drug treatment. The general view of prison drug treatment is that it has changed for the better but that this change is slow.
“My experience with prison services is they are trying … it’s just huge … the whole prison is” (Participant 6, Age 37)
4.6.1 Changes in Prison Drug Treatment
Participants described the early introduction of interventions, including detoxification in the 1990s.
“There was no maintenance in prisons at the time, no methadone maintenance … everyone went in and got a six day detox” (Participant 6, Age 37)
Another participant shared his experience of the late 1990s and noted how significant it was for the Irish Prison Service to acknowledge the scale of the drugs problem.
“I got a two week crash course of 87.5 mils of phy [physeptone]. Now this was before the Medical Unit … so you’d do a detox over two weeks … It was a massive step forward for the Irish Prison Service to acknowledge the drugs problem. It was huge because up until then it was ‘turn a blind eye’ approach to it”. (Participant 5, Age 39)
Around 2000, the Irish Prison Service began the introduction of limited methadone maintenance.
“My experience began in 1999. There was no real monitoring or criteria in those first few years … but it was maybe late 2000 … that you’d notice things beginning to shift.” (Participant 5, Age 39)
4.6.2 Impact of Policy
The 2006 Policy and Strategy on Drugs of the Irish Prison Service was mentioned by one participant. From his responses, he views the Policy and Strategy, not as an abstract document detached from reality, but rather as a document which impacts on the lives of prisoners. He made an interesting point that, even though the focus of this research is the perspectives of ex-prisoners, that there are other perspectives, in particular, the political perspective, which cannot be ignored.
“In any of this you can’t forget the bigger picture … staff resistance … that’s one perspective. Another perspective is what you are looking at. But there’s the political perspective too and you can never ignore that because when politics and prisons mix, the heavy hand falls”. (Participant 5, Age 39)
4.6.3 Slow change
Changes in prison drug treatment have been definite but slow. A general comment on the change in prison drug treatment was expressed which praised the Irish Prison Service for change, even if the change is somewhat slow.
“The IPS [Irish Prison Service] have moved from the stone-age in the 90s. It’s a big organization and some of it seems half-hearted and slow, but it is moving and that’s something you have to give credit to. I know what it’s like and in some ways things don’t have to change, but they have changed and continue to change, it’s just that it goes so slowly.” (Participant 5, Age 39) One participant was clear in his view that the slow-change and lack of funding would not be acceptable for other institutions but that because it was prison, then there was no political or public appetite to speed things up.
“If the Minister goes tomorrow and looks for a million euro for Crumlin children’s hospital and somebody else goes looking for a million euro for addiction services you can rest assure that the children will get it.”
(Participant 4, Age 38)
4.6.4 Role of leadership
The impact of specific personnel in leadership was mentioned as having a strong influence on the direction and pace of change. The current Director General of the Irish Prison Service was appointed in 2011.
“the new head of the prison service was the former head of Probation, Michael Donnellan … he’s a big advocate for prisoners change, people changing in prison, people getting out and starting their lives…he also brought single cells back into Mountjoy…that was a big thing”
(Participant 7, Age 34)
This influence of leadership on change is further reflected in a more rehabilitative approach to prison.
“Prison in Ireland is changing a bit now with the different people involved in IPS. They are seeing a more rehabilitation side of approaching prison rather than the corrective side … they seem to be putting more emphasis on rehabilitation and programmes now … they realize it’s a revolving door so they have to stop it somehow”. (Participant 7, Age 34)
4.7 Attitude and Motivation
The fifth theme is attitude and motivation. This theme was mentioned as an essential part of responding to prison drug treatment. The question put to participants was to do with how prison drug treatment affected their life. The theme indicated how an individual’s willingness to take responsibility for their own recovery played an important role in prison drug treatment.
4.7.1 Desire to change
It was clear through each interview that all the participants had a desire for a life free from chaotic drug using and free from the negative effects of substance misuse. The supports in prison were appreciated as a necessary tool in achieving this.
“All I know is that without supports, fellas will keep going around in cycles and that’s the same for the prison service too, just keep going around and round.” (Participant 5, Age 39)
An improvement in the attitude of participants who engaged with prison drug treatment helped in improving relations with prison staff. Although prison drug treatment could be quite stressful for the participant, it was acknowledged as contributing to making life easier in prison. It was evident from the comments of participants that an individual’s recovery was a hard-earned achievement.
“I became a model prisoner. I had only 2 or 3 reports. I learned to behave. I got clean and good. But it was stressful, fuckin stress. The body has to readjust”. (Participant 2, Age 35)
4.7.2 Honesty and Integrity
The importance of being genuine and honest in one’s attitude was seen as a positive support in achieving treatment objectives. Individuals benefited from those around them being genuine.
“Stick with people that are kind of genuine…and who want to reach their goals because that’s a huge part of it” (Participant 6, Age 37)
It was also important to be honest with oneself.
“It’s a whole lifestyle change…the cliché ‘people, places and things’ need to change….you can’t lie to yourself” (Participant 6, Age 37)
4.7.3 Belief in Change
Belief for participants that positive change was possible in relation to substance misuse often arose in the period leading up to the release date from prison. The impending release date served as a motivation to change and prepare for life after prison.
“I was coming up to the two year mark before I’d get out and I said to myself that I didn’t want to be the same person leaving prison as I was when I went it. That was an important marker for me”. (Participant 5, Age 39)
While the shortage of prison drug treatment services would normally have had a detrimental effect on individuals who did not secure a place, for one individual, it was this shortage in services that moved him to change.
“The change for me came through myself. And it came through myself because either the services were not there or the services that were there were overwhelmed and unable to deal with all the people needing it”. (Participant 5,Age 39)
4.7.4 Attitude towards prison drug treatment
When participants were asked what their general attitude was towards prison drug treatment and whether they would recommend it, they expressed positive responses.
“Anything that’s positive in prison whether it be drug rehabilitation, education, avail of it because they are the tools to change.”
(Participant 7, Age 34)
The importance of being proactive in one’s own recovery helped participants to utilise the services available and also to reach out to particular individuals for support.
“If you’re in Mountjoy and you’re serious…I would definitely encourage following a programme…and it’s up to you to kind of advocate on your behalf and get…Probation or a teacher in the school or someone to advocate on your behalf. And at the end of the day you are the only one who will make that
change.” (Participant 7, Age 34)
Partnership between the individual and services ensured that both parties could achieve their goals together. However, the active participation of the individual seeking prison drug treatment is essential.
“If you are strong in your will and your conviction the services will come around you; you won’t have to go looking for them because they’ll see it in you that you want to change”. (Participant 7, Age 34)
One participant explained succinctly that the biggest obstacle for him in prison drug treatment was his own internal struggle with addiction.
“(the biggest obstacle was) not wanting to let go of my addiction that I loved so much”. (Participant 2, Age 35)
The general attitude and belief of participants towards prison drug treatment could be summed up in the following quote:
“You don’t get anything in life on a plate. Prison drug treatment isn’t the perfect package, but what is? You’ve gotta keep at it til you get a breakthrough. We’ve all been through times of not knowing where life is going or what’s going on. Yeah, where we are in life, part of it can be blamed on upbringing and not having enough of support and care as a child but the older you get, you realize that you can make changes”. (Participant 5, Age 39)
4.8 Accountabilit
The sixth theme is accountability. The issue of accountability arose in each interview. During the interview process, when participants mentioned an issue that they were unhappy about, the interviewer asked if they had made a formal complaint. It was generally accepted by participants that prisoners had very little influence over decisions made about them and that there was no satisfactory recourse to resolve their complaints.
One reason given for not registering a complaint was because participants perceived that it could adversely affect their chances of securing a place on a prison drug treatment programme.
“Because of the shortage of space, you were in no bargaining position to be complaining about anything in prison…So at the end of the day you couldn’t sit there and bang the drum ‘well I want this and I want that’ because they’d just tell you to fuck off”. (Participant 7, Age 34)
The securing of an appointment with a psychologist for this participant seemed to be secured in an arbitrary fashion. Having been unsuccessful in his own attempt to secure an appointment, after mentioning it informally to a teacher in the prison he was given an appointment almost immediately.
“I was three years into my sentence but there was no psychologist available to meet me…but there was a teacher and I mentioned what was going on for me in passing, just in conversation, and then out of nowhere she got an appointment for me for the next week”. (Participant 5, Age 39)
Some participants were left in a predicament because they were not accepted for detoxification and neither could they sustain a regular drug habit because of the lack of regular supply. This had serious effects on the participants including withdrawals.
“I was refused a detox … I couldn’t even lift a snooker cue (I was so weak) … It was the worst experience in prison…caught between a rock and a hard place – not on prison drug treatment and not getting regular supply.” (Participant 2, Age 35)
The limited resources of prison drug treatment impacted on some participants who wanted detoxification or a ‘taper’, but instead they were offered methadone maintenance which they declined. The participants had a profound discomfort with the methadone maintenance. This resulted in one participant going into withdrawals and managing his own detoxification.
“I didn’t want to go cold turkey but it was the only way or else go on methadone. I was serious about getting clean and getting my head straight for when I’d leave prison. So a taper would have been better, come off gear bit by bit, in my own time.” (Participant 3, Age 32)
4.9 Conclusion
This chapter presented the main findings from the seven interviews conducted with participants under the aims of this research. The six themes provide data for a discussion on the findings, which will be the subject of the next chapter.
CHAPTER FIVE: DISCUSSION
5.1 Introduction
This chapter discusses the main findings from the research conducted with the seven participants. From the review of literature, and the seven interviews which were conducted, it is clear that prison drug treatment is a complex topic, with many perspectives from which to view it. This chapter engages the literature review and the findings from the interviews in a discussion so that, through the discussion, another layer of understanding is established.
5.2 Profile of prisoners
The profile of prisoners in general is one of socio-demographic disadvantage. It is clear from this study that this is the case internationally and in Ireland and also among the seven participants. The experience of prison adds to that disadvantage in different ways, which includes the lack of ‘equivalence of care’ in prison drug treatment. Bauman (1998) is clear that prisons are deeply connected to the segregation of unwanted groups through the process of ‘prizonisation’. While Cohen (2001) explains the denial of Society around this knowledge, the reality is that prison drug treatment cannot ignore the socio-economic and educational disadvantage of the prisoner profile. The profile of prisoners highlights the potential that prisons have in helping people recover from disadvantage. Participants in this study identified how prison drug treatment was an important support for them in their journey towards a life free from chaotic drug use. An integrated understanding of all aspects of the individual’s life is an essential feature of prison drug treatment and will note the importance of remedial work in areas such as literacy, emotional development and employability.
5.3 Prison Environment
The impact of the prison environment is recognised throughout this study as being a significant feature of prison drug treatment. Security is the over-arching influence on all aspects of prison and prison drug treatment. The debate as to whether or not prison is the correct environment for prison drug treatment raises deeper questions of the relationship between drugs, crime and society, which are beyond the limits of this study. However, it is clear both from the literature and the interviews that prison adds to the challenges of drug treatment. The negative aspects of the prison environment are often easier to identify. These include boredom, violence, and the presence of drugs. The presence of drugs can create a tense atmosphere and can also undermine the integrity of therapy groups. In this study it was surprising to hear participants identify the benefits of the prison environment. For some participants, their time in prison was a time when they were drug-free for a significant period. This was a considerable achievement. Drug-free wings contributed in a large way to providing a supportive environment, indicating the strong influence the environmental setting can have. Participants commented on how more content they were in drug-free wings because of the supportive climate. While it a a drug-free environment would require an increase in repressive measures without guaranteeing a reduction in supply, the continued development of drug-free areas with aftercare is a realistic response to the needs of individuals who are prepared to engage with prison drug treatment.
5.4 Healthcare
Prison drug treatment as a healthcare strategy has developed over the last thirty years. The gap between what is available in the community and in the prison remains a noticeable shortcoming. For as long as that gap persists, the human rights of prisoners are infringed upon. While the difference between countries in Europe can hamper
comparisons, the move in some countries, towards giving responsibility for prison healthcare to the structure which is responsible for the community, is an interesting trend. It has the potential to improve healthcare and prison drug treatment, while also moving closer to achieving ‘equivalence of care’. However, it has the potential to deflect from other factors relevant to the individuals rehabilitation such as social, behavioural and psychological needs. The medicalising of the needs of an individual can result in compartmentalisation where there is the potential to avoid other needs such as addressing socio-demographic disadvantage. In addition to the move toward integrating prison and community healthcare on a European level, a common instrument could assist in the measuring of effectiveness of prison drug treatment. This would counteract the current situation where there is a variety of data collection and methodologies used which produces data which is incomplete.
5.5 Delivery of prison drug treatment
What was surprising from the interviews with participants is that they made limited critique of the control and sanctions within prison. They were not so concerned about prison drug treatment itself but rather assessed their situation in prison, with reference to their future and return to the community. While empirical research can go into a deep analysis and examination of the content of drug treatment programmes, from the perspective of ex-prisoners in this study what was of greater concern to them was the manner in which treatment was actually delivered. There was also a considered understanding from participants towards the complexity involved in prison drug treatment and the limitations on staff. This appreciation from participants indicates an opportunity to strengthen relationships between staff and participants for the development of services.
5.6 Attitude and Motivation
Another surprising revelation was to do with obstacles to prison drug treatment of which there are many, such as access, availability of illicit drugs, and limited resources. Participants, however, were frank in stating that the main obstacle to prison drug treatment was the internal disposition of the participant. This degree of honesty, self-reflection, and maturity of participants was a constant measure of their engagement with this study.
What also emerged from this study is the challenge posed by limited resources in prison drug treatment such as shortage of spaces. While some participants were creative in adapting to this through self-prescribed approaches to drug treatment, other participants clearly suffered through unsupervised withdrawals. This raises the need for on-going review and evaluation of prison drug treatment, which is already part of the Irish Prison Drug Strategy (2006). What emerges through this study is the multiple layers of challenges which participants had to deal with. Although prison drug treatment was a mixed experience for participants, they acknowledged that it was an important service for them in helping them to become drug-free.
5.7 Accountability
Accountability was a strong theme amongst all participants. While there is a complaints mechanism in the Irish Prison Service, participants did not believe that there was any point in raising a complaint. Participants felt that their concern would not be taken seriously, that there would be negative repercussions for them, and that it was much easier to simply tolerate whatever was at issue. Accountability has been acknowledged by academics as one of the most fundamental difficulties within the Irish Prison Service. Accountability is an even more acute requirement, given the closed nature of prisons, and the power differential between prisoners and staff. For the legitimacy and integrity of prisons in general, and of the prison drug treatment in particular, there needs to be a system of strong and independent oversight which has the confidence of staff and in particular of prisoners.
5.8 Contribution of this study
What is clear from this study is that the number of participants is not large enough to draw generalisations for the whole population who use prison drug treatment in Ireland. It is not possible, therefore, to establish how representative these perspectives are. In any case, while the perspective of ex-prisoners is not the definitive statement on prison drug treatment, it offers an important insight into some experiences of prison
drug treatment. The contribution made by this study is the perspectives of ex-prisoners on prison drug treatment. It contributes important information to the literature of prison drug treatment, such as the challenges for prison drug treatment, the delivery of services and social relations. Through the perspectives of ex-prisoners, the researcher was able to uncover experiences which gave insight into treatment modalities, attitudes, and the prison environment. The perspective of ex-prisoners also challenges assumptions about what is involved in prison drug treatment.
CHAPTER 6: CONCLUSION AND RECOMMENDATIONS
Prison drug treatment is a complex subject which has received a modest amount of research, with less research still on user-perspectives. It is a topic which affects a significant number of people in prisons across Europe. There are many perspectives from which to explore prison drug treatment. The findings of this study arise from the perspectives of ex-prisoners but cannot be applied in general across Irish prisons because of the small sample. This study has looked at the European and Irish situation with regard to prison drug treatment. It has highlighted the socio-demographic background of prisoners, the environmental impact of the prison, the efficacy and modality of prison drug treatment, prison drug treatment as a healthcare strategy, accountability, and the need for regular review and evaluation. It has collected data from seven participants who have experience of prison drug treatment in Ireland and, from that, six themes developed. The discussion chapter has considered these themes, along with the literature review, with a number of recommendations being made.
In light of the information of this study, the researcher makes the following recommendations in relation to prison drug treatment in Ireland.
• Develop research in the area of prison drug treatment in Ireland and, in
particular, from user-perspectives.
• Ensure that there is ongoing monitoring, review and evaluation of prison drug
treatment by the Irish Prison Service.
• Improve access to and ‘throughcare’ in prison drug treatment services.
• Strengthen the structures for accountability within the Irish Prison Service.
• Consider an integrated approach for prison drug treatment across Europe.
This study has countered in a small way the lack of user-perspectives on prison drug treatment. The findings are enriched by interviews with seven participants who have experience of prison drug treatment. Their insights were crucial in shaping this study. Prison drug treatment in Ireland has developed slowly over the last twenty years. For many different reasons though, it does not meet all of the needs of prisoners. The researcher’s hope is that, in another twenty years, an exploratory study of ex-prisoners perspectives on prison drug treatment will reveal an easier pathway to recovery.
REFERENCES
Aebi, M. F. & Delgrande, N. (2015). SPACE I – Council of Europe Annual Penal
Statistics: Prison Populations. Survey 2013. Strasbourg: Council of Europe.
Allwright, S., Barry, J., Bradley, F., Long, J., & Thornton, L. (1999). Hepatitis B,
hepatitis C and HIV in Irish prisoners: Prevalence and risk. Dublin: The
Stationery Office.
Allwright, S., Bradley, F., Long, J., Barry, J., Thornton, L., & Parry, J. V. (2000).
Prevalence of antibodies to hepatitis B, hepatitis C and HIV and risk factors in
Irish prisoners: Results of a national cross sectional survey. British Medical
Journal, 321, 78-82.
Al-Tayyib, A. A., & Koester, S. (2011). Injection drug users‘ experience with and
attitudes toward methadone clinics in Denver, CO. Journal of substance abuse
treatment, 41(1), 30-36.
Baltieri, D. A. (2014). Predictors of drug use in prison among women convicted of
violent crimes. Criminal Behaviour and Mental Health, 24(2), 113-128.
Barry, J., Darker, C., Thomas, D., Allwright, S., & O’Dowd, T. (2010). Primary
medical care in Irish prisons. BMC Health Services Research, 10(1), 74.
Bauman, Z. (1998). Globalization. New York: Columbia University Press.
Bird, S. M., Fischbacher, C. M., Graham, L., & Fraser, A. (2015). Impact of opioid
substitution therapy for Scotland’s prisoners on drugs-related deaths soon after
prisoner-release. Addiction.
Boys, A., Farrell, M., Bebbington, P., Brugha, T., Coid, J., Jenkins, R & Taylor, C.
(2002). Drug use and initiation in prison: results from a national prison survey
in England and Wales. Addiction, 97(12), 1551-1560.
Bridle, C., Murphy, S., Salmon, D., Powell, J., Orme, J., & De Viggiani, N. (2004).
Healthcare needs analysis: an exploratory study of healthcare professionals‘
perceptions of healthcare services at HMP Eastwood Park, South
Gloucestershire.
Bryman, A. (2012). Social research methods. Oxford university press.
Burnett, C. (2009). Research into literacy and technology in primary classrooms: an
exploration of understandings generated by recent studies. Journal of
Research in Reading, 32(1), 22-37.
Carpentier, C., Royuela, L., Noor, A., & Hedrich, D. (2012). Ten years of monitoring
illicit drug use in prison populations in Europe: issues and challenges. The
Howard Journal of Criminal Justice, 51(1), 37-66.
Case of McGlinchey and others v. The United Kingdom (application number
50390/99). Accessed at
http://hudoc.echr.coe.int/sites/eng/pages/search.aspx?i=001-61058 on 8th June
2015.
Cavadino, M., & Dignan, J. (2007). The penal system: An introduction. 4th ed.
London: Sage.
Clausen, T. (2015). Coherent long-term treatment approaches–superior in the treatment
of opioid dependence. Addiction, 110(6), 1006-1007.
Cohen, S., Taylor, L. (1972) Psychological Survival: The Experience of Long-Term
Imprisonment. Harmondsworth: Penguin Books.
Cohen, S. (2001). States of Denial: Knowing about Atrocities and Suffering. Malden,
MA: Blackwell Publishers.
Comptroller and Auditor General. (2009). Drug addiction treatment and rehabilitation.
Special report, Value for Money 64. Accessed 8th June 2015 at
http://audgen.gov.ie/documents/vfmreports/64_Drug_Addiction_and_Rehab.p
df
Costley, C., Elliott, G. C., & Gibbs, P. (2010). Doing work based research:
Approaches to enquiry for insider-researchers. London: Sage.
Council of Europe. (2011). Report to the government of Ireland on the visit to Ireland
carried out by the European Committee for the prevention of torture and
inhuman or degrading treatment or punishment (CPT). Strasbourg: Council of
Europe.
Council of Europe. (2006). Committee of Ministers to Member States on the European
Prison Rules. Committee of Ministers Recommendation (2006)2. Strasbourg:
Council of Europe.
Council of Europe. (1993). Report to the government of Ireland on the visit to Ireland
carried out by the European Committee for the prevention of torture and
inhuman or degrading treatment or punishment (CPT). Strasbourg: Council of
Europe.
Council of Europe. (1998). Ethical and Organisational Aspects of Health Care in
Prison. Committee of Minsters Recommendation No. R (98) 7. Strasbourg:
Council of Europe.
Creswell, J. W. (1994). Qualitative and quantitative approaches and Mixed Methods
Approaches. Sage Publications.
Creswell, J. W. (2009). Research Design: Qualitative, Quantitative, and Mixed
Methods Approaches. 3rd Edition. Los Angeles: Sage Publications, Inc.
Creswell, J. W. (2011). Controversies in mixed methods research. The Sage handbook
of qualitative research, 4, 269-284.
Crewe, B. (2006) The Drugs Economy and the Prisoner Society. In Jewkes, Y. and
Johnston, H. eds. Prison Readings: A Critical Introduction to Prisons and
Imprisonment. Devon: Willan Publishing.
Dara, M., Acosta, C. D., Melchers, N. V. V., Al-Darraji, H. A., Chorgoliani, D., Reyes,
H. & Migliori, G. B. (2015). Tuberculosis control in prisons: current situation
and research gaps. International Journal of Infectious Diseases, 32, 111-117.
Department of Justice (2014). Strategic Review of Penal Policy. Dublin
Denscombe, M. (2010a). Ground rules for social research. Maidenhead: Open
University Press.
Denscombe, M. (2010b). The good research guide for small scale social research
projects. Maidenhead: Open University Press.
Dillon, L., (2001). Drug use among prisoners: An exploratory study. Dublin: The
Health Research Board.
Dolan, K., Moazen, B., Noori, A., Rahimzadeh, S., Farzadfar, F., & Hariga, F. (2015).
People who inject drugs in prison: HIV prevalence, transmission and
prevention. International Journal of Drug Policy, 26, S12-S15.
Drummond, A., Codd, M., Donnelly, N., McCausland, D., Mehegan, J., Daly, L. and
Kelleher, C. (2014). Study on the prevalence of drug use, including
intravenous drug use, and blood-borne viruses among the Irish prisoner
population Technical Report. Dublin: National Advisory Committee on Drugs
and Alcohol.
Elger, B. S., Handtke, V., & Wangmo, T. (2015). Informing patients about limits to
confidentiality: a qualitative study in prisons. International journal of law and
psychiatry.
European Monitoring Centre for Drugs and Drug Addiction (2001) Annual report on
the state of the drugs problem in the European Union. Luxembourg:
Publications Office of the European Union.
European Monitoring Centre for Drugs and Drug Addiction (2012) Annual Report
2012: the state of the drugs problem in Europe. Luxembourg: Publications
Office of the European Union.
European Monitoring Centre for Drugs and Drug Addiction (2012) Prisons and drugs
in Europe: the problem and responses. Luxembourg: Publications Office of
the European Union.
Foddy, W. (1993). Constructing questions for interviews.
Frank, V. A., Dahl, H. V., Holm, K. E., & Kolind, T. (2015). Inmates’ perspectives on
prison drug treatment: A qualitative study from three prisons in Denmark.
Probation Journal.
Garland, D. (2001). The Culture of Control: Crime and Social Control in
Contemporary Society. Chicago: University of Chicago Press.
Gelo, O., Braakmann, D., & Benetka, G. (2008). Quantitative and qualitative research:
Beyond the debate. Integrative psychological and behavioral science, 42(3),
266-290.
Giertsen, H., Nylander, P. Å., Frank, V. A., Kolind, T., & Tourunen, J. (2015).
Prisoners’ experiences of drug treatment and punishment in four Nordic
countries. Nordic Studies on Alcohol and Drugs, 32(2), 145-164.
Godfrey, C., Stewart, D., & Gossop, M. (2004). Economic analysis of costs and
consequences of the treatment of drug misuse: 2-year outcome data from the
National Treatment Outcome Research Study (NTORS). Addiction, 99(6),
697-707.
Hamilton, L., Koehler, J. A., & Lösel, F. (2014). Treatment Programmes for Substance
Abusing Offenders in Europe: A Survey of Routine Practice. European
Journal on Criminal Policy and Research, 1-14.
Harding, R. (2007) Inspecting Prisons. In Jewkes, Y. ed. Handbook on Prisons. Devon:
Willan Publishing.
Herbert, K., Plugge, E., Foster, C., & Doll, H. (2012). Prevalence of risk factors for
non-communicable diseases in prison populations worldwide: a systematic
review. The Lancet, 379(9830), 1975-1982.
Herrick, L. (2009) Prisoners’ Rights. In Kilkelly, U. ed. ECHR and Irish Law. Bristol:
Jordans.
Hucklesby, A., & Wilkinson, C. (2001). Drug misuse in prisons: Some comments on
the prison service drug strategy. The Howard Journal of Criminal Justice,
40(4), 347-363.
Inspector of Prisons (2011) Report on an inspection of Limerick Prison by the
Inspector of Prisons, Judge Michael Reilly, 25 November 2011. Tipperary:
Office of the Inspector of Prisons.
Irish Prison Service (2006) Keeping drugs out of prisons: drugs policy and strategy.
Dublin: Irish Prison Service.
Irish Prison Service (2014) Annual Report 2014 [online] Available from:
http://www.irishprisons.ie/images/pdf/ar2014_english.pdf [Accessed 2nd
September 2015]
Irish Prison Service (2000). Report of the steering group on prison based drug
treatment services. Dublin: Department of Justice, Equality and Law Reform.
Irish Prison Service. (2008). Drug treatment Clinical Policy. Irish Prison Service,
Dublin.
Israel, M., & Hay, I. (2006). Research Ethics for Social Scientists. London: Sage.
Jordan, A. (2010). Lights out on prison healthcare. Medical Independent 10th June.
Available from:
http://www.medicalindependent.ie/page.aspx?title=lights_out_on_prison_heal
thcare [Accessed 14th August 2015].
Punch, K. F. (2005). 2nd Edition. Introduction to Social Research–Quantitative &
Qualitative Approaches. London: Sage.
King, R. D., & Wincup, E. (2000). Doing Research on Crime and Criminal Justice.
Oxford: Oxford University Press.
Koehler, J. A., Humphreys, D. K., Akoensi, T. D., Sánchez de Ribera, O., & Lösel, F.
(2014). A systematic review and meta-analysis on the effects of European
drug treatment programmes on reoffending. Psychology, Crime & Law, 20(6),
584-602.
Koester, S., Anderson, K., Hoffer, L., (1999) Active heroin injector’s perceptions and
use of methadone treatment. Substance Use and Misuse, 34(14): 2135-2153.
Kolind, T. (2007) Form or content: The application of user perspectives in treatment
research. Drugs: Education, Prevention and Policy, 14(3): 261-275.
Kolind, T., Frank, V.A., Lindberg, O., Tourunen, J. (2013) Prison-based drug treatment
in Nordic political discourse: An elastic discursive construct. European
Journal of Criminology, 10, 659-674.
Kothari, G., Marsden, J., & Strang, J. (2002). Opportunities and obstacles for effective
treatment of drug misusers in the criminal justice system in England and
Wales. British Journal of Criminology, 42(2), 412-432.
Kvale, S. (1996). InterViews. An introduction to qualitative research writing.
California: Sage.
Liebling, A. and Maruna, S. (2005). ‘Introduction: The Effects of Imprisonment
revisited’ In: Liebling, A. and Maruna, S. eds. The Effects of Imprisonment.
Devon: Willan Publishing.
Liebling, A., Durie, L., Stiles, A., & Tait, S. (2005). ‘Revisiting prison suicide: the role
of fairness and distress’ In: Liebling, A. and Maruna, S. eds. The Effects of
Imprisonment. Devon: Willan Publishing.
Lincoln, Y. S., & Denzin, N. K. (2003). Turning points in qualitative research: Tying
knots in a handkerchief. Rowman Altamira.
Long, J., Allwright, S., & Begley, C. (2004). Prisoners’ views of injecting drug use and
harm reduction in Irish prisons. International Journal of Drug Policy, 15(2),
139-149.
Lyons, S., Walsh, S., Lynn, E. and Long, J. (2010). Drug-related deaths among
recently released prisoners in Ireland, 1998 to 2005, International Journal of
Prisoner Health. 6(1), 26–32.
McIlwraith, F., Hickey, S. and Alati, R. (2012), Benzodiazepine update: alprazolam
and other benzodiazepine use among people who inject drugs, National Drug
and Alcohol Research Centre, The University of New South Wales, Sydney
McIntosh, J., & Saville, E. (2006). The challenges associated with drug treatment in
prison. Probation Journal, 53(3), 230-247.
MacNamara, C., & Mannix-McNamara, P. (2014). Placing the promotion of health and
well being on the Irish prison agenda-the complexity of health promotion in
Irish prisons. Irish Journal of Applied Social Studies, 14(1), 6, 49-59.
Malloch, M., & McIvor, G. (2013). Criminal justice responses to drug related crime in
Scotland. International Journal of Drug Policy, 24(1), 69-77.
Møller, L., Gatherer, A., Jürgens, R., Stöver, H., & Nikogosian, H. (2007). Health in
prisons: a WHO guide to the essentials in prison health. WHO Regional
Office Europe.
Montanari, L., Royuela, L., Pasinetti, M., Giraudon, I., Wiessing, L., & Vicente, J.
(2014). 13. Drug use and related consequences among prison populations in
European countries. Prisons and Health, 107.
Moore, G., McCarthy, P., MacNeela, P., MacGabhann, L., Philbin, M., &
Proudfoot, D. (2004). A review of harm reduction approaches in
Ireland and evidence from the International literature. Stationery
Office.
Moore, P. (2007) An exploratory Study of Young Offenders’ Views
Concerning Drugs, Crime and Drug Policy. European Monitoring
Centre for Drugs and Drug Addiction.
Mountjoy Prison Visiting Committee (2012) Mountjoy Prison annual report
2011. Dublin: Department of Justice and Equality.
National Advisory Committee on Drugs (2006) Research Outcome Study in Ireland –
12-month Outcomes. Dublin: Stationery Office.
Neale, J. (1998) Drug users’ views of drug service providers. Health and Social Care
in the Community, 6(5), 308-317.
Notley, C., Maskrey, V., Holland, R. (2012). The needs of problematic drug misusers
not in structured treatment – a qualitative study of perceived treatment barriers
and recommendations for services. Drugs: Education, Prevention, and Policy,
19(1), 40-48.
Niveau, G. (2007). Relevance and limits of the principle of “equivalence of care” in
prison medicine. Journal of medical ethics, 33(10), 610-613.
O’Grada, C. (2010). Staff perspectives on drug treatment in prison. Doctoral
Dissertation: TCD.
O’Mahony, P. (2002). Criminal Justice in Ireland. Dublin: Institute of Public
Administration.
Obstbaum, Y., & Tyni, S. (2015). Who receives substance abuse treatment in the ‘real
world’of the prison? A register-based study of Finnish inmates. Journal of
Scandinavian Studies in Criminology and Crime Prevention, 16(1), 76-96.
Pont, J., Stöver, H., & Wolff, H. (2012). Dual loyalty in prison health care. American
Journal of Public Health, 102(3), 475-480.
Ramsay, M. (2003) Prisoners Drug Use and Treatment. Research Study No. 267.
London: Home Office, Development and Statistics directorate.
Redondo, S., Sanchez-Meca, J., & Garrido, V. (1999). The influence of treatment
programmes on the recidivism of juvenile and adult offenders: An European
meta-analytic review. Psychology, Crime and Law, 5(3), 251-278.
Ritter, C., Broers, B., & Elger, B. S. (2013). Cannabis use in a Swiss male prison:
Qualitative study exploring detainees’ and staffs’ perspectives. International
Journal of Drug Policy, 24(6), 573-578.
Rogan, M. (2014). Prison Law. Dublin: Bloomsbury Professional.
Rubin, J. R., & Rubin, I. (2005). Qualitative interviewing: The art of hearing data.
California: Sage.
Ryberg, J. (2013). Is Coercive Treatment of Offenders Morally Acceptable? On the
Deficiency of the Debate. Criminal Law and Philosophy, 1-13.
Sarantakos, S. (2005). Social Research. 3rd ed. Hampshire: Palgrave MacMillan
Seddon, T. (2007). Coerced drug treatment in the criminal justice system Conceptual,
ethical and criminological issues. Criminology and Criminal Justice, 7(3),
269-286.
Stebbins, R. A. (2001). Exploratory research in the social sciences (Vol. 48). Sage
Publications.
Stoever, H. (2002). Drug substitution treatment and needle exchange programs in
German and European prisons. Journal of drug issues, 32(2), 573-596.
Stöver, H., & Michels, I. I. (2010). Drug use and opioid substitution treatment for
prisoners. Harm Reduction Journal, 7(1).
Stöver, H., & Kastelic, A. (2014). Drug treatment and harm reduction in prisons.
Prisons and Health, 113.
Strang, J. (2015). Death matters: understanding heroin/opiate overdose risk and testing
potential to prevent deaths. Addiction, 110(S2), 27-35.
Swogger, M. T., Conner, K. R., Walsh, Z., & Maisto, S. A. (2011). Childhood abuse
and harmful substance use among criminal offenders. Addictive behaviors,
36(12), 1205-1212.
Thorseth, M. (Ed.). (2003). Applied Ethics in Internet Research. Programme for
Applied Ethics, Norwegian University of Science and Technology.
Trondheim: NTNU University Press.
UN Committee on Economic, Social and Cultural Rights (CESCR). (2000). General
Comment No. 14: The Right to the Highest Attainable Standard of Health.
UN General Assembly, International Covenant on Economic, Social and Cultural
Rights, 16 December 1966, United Nations, Treaty Series, vol. 993, p.
3, available at: http://www.refworld.org/docid/3ae6b36c0.html [accessed 8
June 2015]
UN General Assembly, Basic Principles for the Treatment of Prisoners: resolution /
adopted by the General Assembly, 28 March 1991, A/RES/45/111, available
at: http://www.refworld.org/docid/48abd5740.html [accessed 8 June 2015]
Vandam, L. (2009), Patterns of drug use before, during and after detention: a review of
epidemiological literature. In Cools, M. (editor), Contemporary issues in the
empirical study of crime. Maklu, Antwerp.
Walmsley, R. (2013). World prison population list (tenth edition). London, England:
Home Office.
World Health Organization (WHO). (1986). Ottawa charta for health promotion.
Geneva: WHO.
Wheatley, M. (2007). Drugs in prison. In Jewkes, Y. ed. Handbook on Prisons. Devon:
Willan Publishing.
Woodall, J. (2011). Social and environmental factors influencing in-prison drug use.
Health Education, 112(1), 31-46.
APPENDICES
Appendix 1: Consent Form
I have read this information sheet and have had time to consider whether to take part in this
study.
I understand that my participation is voluntary (it is my choice) and that I am free to withdraw
from the research at any time without disadvantage. I agree to take part in this research.
I understand that, as part of this research project I will be interviewed for a maximum period of
60 minutes on the topic of my experience of drug treatment in prison.
I understand that my name will not be identified and that it will be changed when the research
is written.
I am voluntarily agreeing to participate in this research.
I agree that the data can be used in the publication of higher degrees, scientific publications.
I understand that the completed research may appear online and in DIT library.
Name of Participant (in block letters):
______________________________________
Signature:_______________________________________________________
Date: / /
Appendix 2: Information Letter
9th July 2015.
To the Director of Project X:
I am writing to you as a post-graduate student in Dublin Institute of Technology. I am conducting research on the experience of ex-prisoners of drug treatment in prison. The research is for a Masters thesis in Criminology. It has received research ethics approval from the Head of School of Languages, Law and Social Sciences, Dr. Kevin Lalor.
I have contacted you as Director of Project X, which is a drug-free community based education
programme in ________________.
My request is to interview six people individually about their perspective on drug treatment in prison. It would be one interview lasting a maximum of 60 minutes. The research is conducted in a confidential way with the exceptions to confidentiality if child protection concerns arise.
The identity of each participant will be changed so as to provide anonymity. Data will be securely stored throughout the research and then destroyed on completion of the study. The use of a digital recorder with permission of the participant would be helpful but not essential.
Taking part in this research would be voluntary and consent can be withdrawn at any time. The completed work may appear in the DIT library and online at www.arrow.dit.ie.
I am available by email on d13122683@mydit.ie for further information and questions. I can also be contacted on
Yours sincerely,
Sean Duggan
Appendix 3: Information Sheet
I am a student in Dublin Institute of Technology (DIT). I am carrying out research and need your help.
The research project is on the views of people, with prison experience, about drug treatment while in prison.
People who take part will be interviewed by me for a maximum period of 60 minutes.
I am interested in your experience, thoughts and opinions. What you say will be treated in confidence. In other words, it will not be passed on to the Gardai or Prison authorities. The one exception is if something arises which indicates that you are a danger to yourself or someone else.
Your anonymity will be respected and your name will not be identified in any published material. Any notes, interview material or other data will be securely stored during the research and then destroyed when the research is complete.
I would like to use a digital recorder during the interview if possible. This is so that I can get everything that is said and not need to take notes. If you would prefer that the interview not be recorded, I can take notes instead.
Taking part in this research is completely voluntary. You have the right and the choice to withdraw at any time. There will be no penalty for withdrawing and your access to services will not be affected.
One risk in taking part in this research is that it could raise some upsetting memories for you. One benefit in taking part is that you will be making an important contribution to the knowledge and understanding of drug treatment in prison.
I can be contacted by email on d13122683@mydit.ie
If you would like to talk to my Supervisor for more details, please contact Dr. Kevin Lalor by
email on kevin.lalor@dit.ie